
Skeleton - PowerPoint PPT Presentation
1 / 74
Title: Skeleton
1
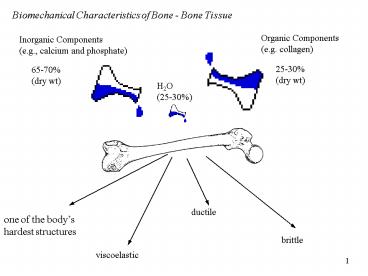
Biomechanical Characteristics of Bone - Bone
Tissue
Organic Components (e.g. collagen)
Inorganic Components (e.g., calcium and phosphate)
25-30 (dry wt)
65-70 (dry wt)
H2O (25-30)
ductile
one of the bodys hardest structures
brittle
viscoelastic
2
Strength and Stiffness of Bone Tissue
evaluated using relationship between applied
load and amount of deformation LOAD -
DEFORMATION CURVE
Bone Tissue Characteristics
Anisotropic
Viscoelastic
Elastic
Plastic
3
Stress Force/Area
Strain Change in Length/Angle
Note Stress-Strain curve is a normalized
Load-Deformation Curve
4
Elastic Plastic responses
- elastic thru 3deformation
- plastic response leads to fracturing
- Strength defined by failure point
- Stiffness defined as the slope of the
- elastic portion of the curve
5
Elastic Biomaterials (Bone)
- Elastic/Plastic characteristics
- Brittle material fails before
- permanent deformation
- Ductile material deforms
- greatly before failure
- Bone exhibits both properties
Load/deformation curves
elastic limit
ductile material
load
brittle material
bone
deformation (length)
6
Anisotropic response behavior of bone is
dependent on direction of applied load
Bone is strongest along long axis - Why?
7
Viscoelastic Response behavior of bone is
dependent on rate load is applied
Bone will fracture sooner when load applied slowly
8
Mechanical Loading of Bone
Compression Tension Shear Torsion
Bending
9
Compressive Loading
Vertebral fractures cervical fractures spine
loaded through head e.g., football, diving,
gymnastics once spearing was outlawed
in football the number of cervical injuries
declined dramatically lumbar fractures weight
lifters, linemen, or gymnasts spine is loaded in
hyperlordotic (aka swayback) position
10
Tensile Loading
Main source of tensile load is muscle tension
can stimulate tissue growth fracture
due to tensile loading is usually an
avulsion other injuries include sprains, strains,
inflammation, bony deposits when the tibial
tuberosity experiences excessive loads from
quadriceps muscle group develop condition known
as Osgood-Schlatters disease
11
Shear Forces created by the application of
compressive, tensile or a combination of these
loads
12
Relative Strength of Bone
13
Bending Forces
Usually a 3- or 4-point force application
14
Torsional Forces
Caused by a twisting force produces shear,
tensile, and compressive loads tensile and
compressive loads are at an angle often see a
spiral fracture develop from this load
15
SKELETON
- axial skeleton
- skull, thorax, pelvis, vertebral column
- appendicular skeleton
- upper and lower extremities
- should be familiar with all major bones
16
Purposes of Skeleton
- protect vital organs
- factory for production of red blood cells
- reservoir for minerals
- attachments for skeletal muscles
- system of machines to produce movement in
- response to torques
17
Bone Vernacular
- condyle
- a rounded process of a bone that articulates with
another bone - e.g. femoral condyle
- epicondyle
- a small condyle
- e.g. humeral epicondyle
18
Bone Vernacular
- facet
- a small, fairly flat, smooth surface of a bone,
generally an articular surface - e.g. vertebral facets
- foramen
- a hole in a bone through which nerves or vessels
pass - e.g. vertebral foramen
19
Bone Vernacular
- fossa
- a shallow dish-shaped section of a bone that
provides space for an articulation with another
bone or serves as a muscle attachment - glenoid fossa
- process
- a bony prominence
- olecranon process
20
Bone Vernacular
- tuberosity
- a raised section of bone to which a ligament,
tendon, or muscle attaches usually created or
enlarged by the stress of the muscles pull on
that bone during growth - radial tuberosity
21
Long Bones
- e.g. femur, tibia
- 1 long dimension
- used for leverage
- larger and stronger in lower extremity than upper
extremity - have more weight to support
22
Short Bones
- e.g. carpals and tarsals
- designed for strength not mobility
- not important for us in this class
23
Flat Bones
- e.g. skull, ribs, scapula
- usually provide protection
24
Irregular Bones
- e.g. vertebrae
- provide protection, support and leverage
25
Sesamoid Bones
- e.g. patella (knee cap)
- a short bone embedded within a tendon or joint
capsule - alters the angle of insertion of the muscle
26
Long Bone Structure
cortical or compact bone (porosity 15)
periosteum outer cortical membrane
endosteum inner cortical membrane
trabecular, cancellous, or spongy, bone
(porosity 70)
27
Long Bone Structure
epiphyseal plate cartilage separating metaphysis
from epiphysis
metaphysis either end of diaphysis filled with
trabecular bone
diaphysis shaft of bone
epiphysis proximal and distal ends of a long bone
28
Biomechanical Characteristics of Bone
Physical Activity
Lack of Activity
Bone Tissue Remodeling/Growth
Gravity
Hormones
Bone Deposits (myositis ossificans)
Age Osteoporosis
29
Longitudinal Bone Growth
- occurs at the
- epiphyseal or
- growth plate
- bone cells are produced on the diaphyseal side of
the plate - plate ossifies around age 18-25 and longitudinal
growth stops
30
Circumferential Bone Growth
- growth throughout the
- lifespan
- bone cells are produced on the internal layer of
the periosteum by osteoblasts - concurrently bone is resorbed around the
circumference of the medullary cavity by
osteoclasts
31
Wolffs Law
Biomechanical Characteristics of Bone
- bone is laid down where needed and resorbed where
not needed - shape of bone reflects its function
- tennis arm of pro tennis players have cortical
thicknesses 35 greater than contralateral arm
(Keller Spengler, 1989) - osteoclasts resorb or take-up bone
- osteoblasts lay down new bone
32
Bone Deposits
- A response to regular activity
- regular exercise provides stimulation to maintain
bone throughout the body
- tennis players and baseball pitchers develop
larger and more dense bones in dominant arm - male and female runners have higher than average
bone density in both upper and lower extremities - non-weightbearing exercise (swimming, cycling)
can have positive effects on BMD
33
Bone Resorption
- lack of mechanical stress
- Calcium (Ca) levels decrease
- Ca removed through blood via kidneys
- increases the chance of kidney stones
- weightless effects (hypogravity)
- astronauts use exercise routines to provide
stimulus from muscle tension - these are only tensile forces - gravity is
compressive
34
(No Transcript)
35
Tip-Toe running pattern
Heel-toe running pattern
36
TVIS Treadmill Vibration Isolation
and Stabilization System
37
Changes in bone over timeEarly Years
- Osgood-Schlatters disease
- development of inflammation, bony deposits, or an
avulsion fracture of the tibial tuberosity - muscle-bone strength imbalance
- growth factor between bone length and muscle
tendon unit (e.g., rapid growth of femur and
tibia places large strain on patellar tendon and
tibial tuberosity) - during puberty muscle development (testosterone)
may outpace bone development allowing muscle to
pull away from bone
38
Changes in bone over timeEarly Years
- overuse injuries
- repeated stresses mold skeletal structures
specifically for that activity - Little Leaguers Elbow
- premature closure of epiphyseal disc
- Gymnasts
- 4X greater occurrence of low back pathology in
young female gymnasts than in general population
(Jackson, 1976)
39
Changes in bone over timeAdult Years
- little change in length
- most change in density
- lack of use decreases density
- DECREASE STRENGTH OF BONE
- activity
- increased activity leads to increased diameter,
density, cortical width and Ca
40
Changes in bone over timeAdult Years
- hormonal influence
- estrogen to maintain bone minerals
- previously only consider after menopause
- now see link between amenorrhea and decreased
estrogen - Female Athlete Triad
41
Changes in Bone Over TimeOlder Adults
- 30 yrs males and 40 yrs females
- BMD peaks (Frost, 1985 Oyster et al., 1984)
- decrease BMD, diameter and mineralization after
this - activity slows aging process
42
Reduced BMD slightly elevated risk of fracture
Osteopenia
Severe BMD reduction very high risk
of fracture (hip, wrist, spine, ribs)
Osteoporosis
Hormonal Factors
Nutritional Factors
Physical Activity
28 million Americans affected 80 of these are
women 10 million suffer from osteoporosis 18
million have low bone mass
43
Osteoporosis
- age
- women lose 0.5-1 of their bone mass each year
until age 50 or menopause - after menopause rate of bone loss increases (as
high as 6.5)
44
Do you get shorter with age?
- Osteoporosis compromises structural integrity of
vertebrae - weakened trabecular bone
- vertebrae are crushed
- actually lose height
- more weight anterior to spine so the compressive
load on spine creates wedge-shaped vertebrae - create a kyphotic curve known as Dowagers Hump
- for some reason mens vertebrae increase in
diameter so these effects are minimized
45
Preventing Osteoporosis
- 13.8 billion in 1995 (38 million/day)
- Lifestyle Choices
- proper diet
- sufficient calcium, vitamin D,
- dietary protein and phosphorous (too much?)
- tobacco, alcohol, and caffeine
- EXERCISE, EXERCISE, EXERCISE
- 47 incidence of osteoporosis in sedentary
population compared to 23 in hard physical labor
occupations (Brewer et al., 1983)
46
Osteoporosis, Activity and the Elderly
Rate of bone loss (50-72 yr olds, Lane et al.,
1990) 4 over 2 years for runners 6-7 over 2
years for controls However - rate of loss jumped
to 10-13 after stopped running suggest
substitute activities should provide high
intensity loads, low repetitions (e.g. weight
lifting)
47
Injury - Repetitive v. Acute Loading
injury tolerance (above this line injury will
occur)
magnitude of loading
frequency of loading
48
Articulations
- junction of 2 bones
- MOTION OCCURS AT A JOINT -- NOT AT A LIMB
- i.e. elbow flexion NOT forearm flexion
49
Classification of joints
- Synarthroses - fibrous joint with little or no
movement - Amphiarthroses - cartilaginous joints with some
motion - Diarthroses - (aka synovial) - freely movable
joint
50
(No Transcript)
51
Joint Classification
- based on
- number of axes of rotation
- number of planes of motion
- e.g. uniaxial -- 1 axis of rotation so 1 plane of
motion
52
Ball and Socket Triaxial e.g., flexion
extension internal external rotation abduction
adduction
Condyloid Biaxial e.g., flexion
extension internal external rotation
53
Pivot uniaxial e.g., supination pronation
Hinge uniaxial e.g., flexion and extension
54
Gliding no axes gliding between 2 flat bones
Saddle biaxial same as condyloid but greater ROM
Ellipsoidal biaxial e.g., flexion
extension abduction adduction
55
Structure of Synovial Joint
- A - articular (hyaline) cartilage (1-7 mm)
- smooth elastic tissue on ends of bone
- 60-80 water
- no blood supply
- absorbs shock, distributes force and provides a
low friction surface
56
Structure of Synovial Joint
- B - fibrous capsule
- very fibrous collagen tissue used to hold bones
together - C - synovial membrane
- lines the joint cavity
- secretes synovial fluid to lubricate and provide
nutrition
NOTE B C combine to form the articular capsule
or joint capsule
57
Structure of Synovial Joint
- D - ligaments
- connect bone-to-bone
- usually restrict ROM at a joint
- tendons (not shown)
- connect muscle-to-bone
A - Joint cavity
58
Other Structures of Synovial Joints
- bursa
- small capsules lined with synovial membranes
- reduces friction between other structures in the
joint - tendon sheaths
- fascia surrounding tendon to reduce friction
between tendon and surrounding structures
Olecranon bursa
Digital synovial sheath
59
Other Structures of Synovial Joints
- articular fibrocartilage
- different from articular cartilage
- takes the form of a fibrocartilaginous disc or
partial disc - distributes load over joint surface
- improve fit of articulating surfaces
- limit slipping of one bone relative to other
- protect periphery of articulation
- lubricate articulation
- absorb shock
60
Arthritis
- Refers to more than 100 different diseases that
affect areas in or around joints. - The disease also can affect other parts of the
body. - Arthritis causes pain, loss of movement and
sometimes swelling. - Affects women more than men
Source Arthritis Foundation www.arthritis.org
61
Osteoarthritis 20.7 million Mostly after age 45
Fibromyalgia 3.7 million Mostly women
Rheumatoid 2.1 million Mostly women
Juvenile Arthritis 285,000 Under age 17
Gout 2.1 million Mostly men
Arthritis
Spondylarthropathies 412,000
Juvenile Rheumatoid Arthritis (JRA) 50,000
Lupus 239,000
Source Arthritis Foundation www.arthritis.org
62
Osteoarthritis (OA), or degenerative joint
disease, is one of the oldest and most common
types of arthritis, characterized by the
breakdown of the joint's cartilage. Cartilage is
the part of the joint that cushions the ends of
bones. Cartilage breakdown causes pain and joint
swelling. With time, there will be limited joint
movement.
- Most commonly affects middle-aged and older
people - Range from very mild to very severe
- Affects hands and weight-bearing joints (e.g.,
knees, hips, feet and back). - OA is not an inevitable part of aging, although
age is a risk factor - Obesity may lead to osteoarthritis of the knees
- Joint injuries due to sports, work-related
activity or accidents may be at increased risk of
developing OA.
Source Arthritis Foundation www.arthritis.org
63
Rheumatoid Arthritis (RA) a systemic disease
that affects the entire body.
- Characterized by the inflammation of the
membrane lining the joint, which causes pain,
warmth, redness and swelling. - The inflamed joint lining, the synovium, can
invade and damage bone and cartilage. - Inflammatory cells release enzymes that may
digest bone and cartilage. - The involved joint can lose its shape and
alignment, resulting in pain and loss of
movement. - The disease usually begins in middle age, but
can start at any age, and affects two to three
times more women than men.
Source Arthritis Foundation www.arthritis.org
64
Location of Tender Points
Fibromyalgia syndrome is a condition with
generalized muscular pain and fatigue that is
believed to affect approximately 3.7 million
people.
- The name fibromyalgia means pain in the muscles
and the fibrous connective tissues (the ligaments
and tendons). The condition is known as a
syndrome because it is a set of signs and
symptoms that occur together. - Fibromyalgia mainly affects muscles and their
attachments to bones. Although it may feel like a
joint disease, it is not a true form of arthritis
and does not cause deformities of the joints.
Fibromyalgia is, instead, a form of soft tissue
or muscular rheumatism.
Source Arthritis Foundation www.arthritis.org
65
Use of Heat or Cold Helpful before and after
exercise Many respond better to cold packs than
to heat
Rest More rest and less activity are needed
during flares and the opposite is true during
periods of improvement.
Medicines (e.g., analgesics, NSAIDS, DMARDS,
Disease Modifying Anti-Rheumatic Drugs)
Exercise (see next slide)
Surgery joint replacement
Arthritis Treatments
Joint Protection Careful use of joints to limit
the pressure on the involved joint Simple and
inexpensive devices available
Use of Heat or Cold Helpful before and after
exercise Many respond better to cold packs than
to heat
- Diet
- Lack of vitamins associated with progression of
OA of the knee - Connection between obesity and OA of the knee
- Diet high in Omega 3 fatty acids may help reduce
inflammation in RA - In general, people with arthritis are urged to
maintain a balanced diet and stay close to their
ideal weight.
- Physical/Occupational Therapy
- recommend and teach prescribed muscle
strengthening and range-of-motion exercises - teach non-medication ways to control pain
- suggest ways to make everyday and work
activities easier
Source Arthritis Foundation www.arthritis.org
66
- Exercise
- Proper exercises performed on a daily basis are
an important part of arthritis treatment. - Exercise to help reduce weight can help prevent
osteoarthritis in the knee. - Proper exercise helps build and preserve muscle
strength, keep joints flexible and help protect
joints from further damage. - Two categories of exercise
- Therapeutic -- Prescribed by a doctor, physical
therapist or an occupational therapist. These
exercises are based on individual needs and are
designed to reach a certain goal. - Recreational -- Includes any forms of movement,
amusement or relaxation that refreshes the body
and mind. These exercises add to a therapeutic
program, but do not replace it. - Three types of exercises
- Range-of-motion -- Moving a joint as far as it
comfortably will go and then stretching it a
little further. Range-of-motion exercises are
designed to increase and maintain joint mobility
that will decrease pain and improve function. - Strengthening -- Increases muscle strength to
stabilize weak joints. These exercises use the
muscle without moving the joint. - Endurance -- This type of exercise includes
walking, swimming, bicycling, jogging, dancing
and skiing. These dynamic forms of exercise
increase endurance, whereas range-of-motion and
strengthening do not. The most common risk in
exercising is injury to joints and muscles. This
usually happens from exercising too long or too
hard, especially if a person has not been active
for some time.
Source Arthritis Foundation www.arthritis.org
67
close-packed vs. loose packed
- close packed position
- maximum contact area
- minimum mobility
- maximum stability
68
Bony Stability (cont.)
- amount of contact area
69
Joint Stability - Connective Tissue
- ligamentous support
70
Properties of Connective Tissue
- elasticity
- ability to return to normal state after stretch
- elastic limit
- stretch beyond this limit will cause permanent
damage - plasticity
- stretched too far such that does not return to
its normal state - ligament sprain (worse than bone fracture)
71
Exercise will help increase the loads a
ligament or tendon can sustain
Sprains result in decrease of joint stability
72
Joint Stability - Muscles
- muscular arrangement
- ability of muscle to provide support
- muscle fatigue
- cruciate rupture more likely when muscle is
fatigued
73
Mobility
- degree to which an articulation is allowed to
move before being restricted by surrounding
tissues - ROM a.k.a. flexibility
74
Stability v. Mobility
- trade-off between stability and mobility
- increase stability decrease mobility
- vice-versa
Recommended
CrystalGraphics Presentations





























