
Endocrine System Disorder - PowerPoint PPT Presentation
Title: Endocrine System Disorder
1
- Endocrine System Disorder
2
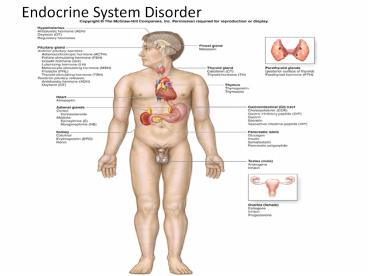
Endocrine System
- The foundations of the endocrine system are the
hormones and glands. As the body's chemical
messengers, hormones transfer information and
instructions from one set of cells to another. - The major glands that make up the human endocrine
system are t hypothalamus - - pituitary
- - thyroid
- - parathyroids
- - adrenals pineal body
- - and the reproductive glands, which include
the ovaries and testes. - The pancreas is also part of this
hormone-secreting system, it is also associated
with the digestive system because it also
produces and secretes digestive enzymes.
3
Pancreas
- The pancreas is a glandular organ that secretes
digestive enzymes (internal secretions) and
hormones (external secretions). In humans, the
pancreas is a yellowish organ about 7 inches
(17.8 cm) long and 1.5 inches. (3.8 cm) wide. - The pancreas lies beneath the stomach and is
connected to the small intestine at the duodenum
4
Pancreas - Functions
- The pancreas contains enzyme producing cells that
secrete two hormones. - The two hormones are insulin and glucagon.
Insulin and glucagon are secreted directly into
the bloodstream, and together, they regulate the
level of glucose in the blood. - Insulin lowers the blood sugar level and
increases the amount of glycogen (stored
carbohydrate) in the liver. - Glucagon slowly increases the blood sugar level
if it falls too low. If the insulin secreting
cells do not work properly, diabetes occurs.
5
Pancreas - Function
- The pancreas also helps neutralize chyme and
helps break down proteins, fats and starch. - Chyme is a thick semi-fluid mass of partly
digested food that is passed from the stomach to
the duodenum. - If the pancreas is not working properly to
neutralize chyme and break down proteins, fats
and starch, starvation may occur. - Conditions of the Pancreas
- Pancreatitis is a condition that affects the
pancreas.
6
Pancreas location anatomically
7
Pancreas
8
Endocrine Disorder
- Diabetes Millitus
- Diabetes Mellitus is a chronic multisystem
disease related to abnormal insulin production,
impaired insulin use, or both. - Insulin is a hormone that helps the glucose get
into the cells to give them energy. With Type 1
diabetes, the body does not make insulin. With
Type 2 diabetes, the more common type, the body
does not make or use insulin well. Without enough
insulin, the glucose stays in your blood.
9
Diabetes Mellitus
- DM is a serious health problem throughout the
world. - Leading cause of end-stage renal disease.
- Adult blindness.
- Non-traumatic limb amputation.
- Major contributing Factor in
- Heart disease and stroke
- Decreased tissue perfusion in D.M. may lead to
cardiovascular disease, hypertension, renal
failure, blindness, and stroke
10
Diabetes Mellitus
- Over time, having too much glucose in blood can
cause serious damage to eyes (retinopathy),
kidneys (nephropathy), and nerves (neuropathy). - Diabetes can also cause
- - heart disease
- - stroke
- - amputation (need to remove a limb).
- - Pregnant women can also get diabetes,
called - gestational diabetes.
11
Current Theories leading to its Etiology
- Genetic
- Autoimmune
- Viral
- Environmental factors (e.g. viral and stress).
- Two Most Common Types
- Type 1 IDDM, Juvenile Diabetes
- Type 2 NIDDM, Adult Onset DM
- Gestational, pre-diabetes, secondary diabetes
12
Diagnostic tests
- Diagnostic criteria
- Two findings (separate days) of one of the
following - Symptoms of DM plus casual plasma
- glucose concentration of greater than 200
- mg/dL ( without regard to time since last
- meal).
- Fasting Blood Glucose greater than 126 mg/dL (8
hour fasting). - Two-hour glucose greater than 200 mg/dL with an
oral glucose tolerance test (10 to 12 hr.
fasting).
13
DM Diagnostic Tests Nursing Intervention
- FBG or FBS ensure client has fasted for 8 hours
prior to the blood draw. Antidiabetic
(hypoglycemic agents) medications should be
postponed until after the level is drawn. - Pre-meal glucose The target is 90 130 mg/dL.
Follow or ensure that the client follow the
procedure for blood sample collection and use of
glucose meter. Supplemental short-acting insulin
maybe prescribed for elevated pre-meal glucose
levels.
14
DM Diagnostic Tests Nursing Intervention
- Oral Glucose Tolerance Test (OGTT) Instruct the
client to consume a balanced diet for the three
days prior to the test. Then instruct the client
to fast for 10 12 hr. prior to the test. - A FBS is drawn at start of the test. The
client - is then instructed to consume a specified
- amount of glucose. BG level or CBG level are
- drawn every 30 min. for 2 hr. Client must be
- assessed for hypoglycemia throughout the
- procedure
15
DM Diagnostic Tests Nursing Intervention
- Glycosylated Hemonglobin (Hgb A1- C)
- - This is used to determine the long-term
- compliance of client to DM treatment
- regimen.
- The target is 4 to 6 Hgb A1-C. HgbA1-C is the
best indicator of average blood glucose for past
120 days. Assist for evaluating treatemtn
effectiveness and compliance.
16
Assessments Sign and Symptoms to look
forStart prioritizing
Type 1 Type 2
Polyuria, polydipsia, polyphagia Polyuria, polydipsia, polyphagia
Weight Loss Obesity
Fatigue Fatigue
Increase frequency of infections Increase frequency of infections
Rapid Onset Gradual Onset
Controlled by exogenous insulin Controlled by Oral hypoglycemic medications and insulin
17
Sign and Symptoms by Glucose Alteration
Hypoglycemia ( equal or less than 50 mg/dL) Hyperglycemia (equal or more than 250 mg/dL)
Cool clammy skin Hot, dry skin
Diaphoresis (sweating) Absence of diaphoresis (absence of sweating)
Anxiety, irritability, confusion, blurred vision Alert to coma ( varies)
Hunger Nausea and vomiting, abdominal pain (with ketoacidosis)
General weakness, seizure ( severe hypoglycemia Rapid deep respiration (Kaussmals breathing) acetone/fruity odor due to ketones this is resulting from Diabetic ketoacidosis
18
Blood Glucose monitors
19
Glucose Continuum
20
Normal Insulin Secretion
21
Insulin Preparations
22
Insulin Pen
23
Insulin Pump
24
Subcutaneous Injection Sites
25
Type 1 DM (Insulin Dependent DM)
- Type 1 diabetes ( Juvenile Diabetes Mellitus)
- When the pancreas fails to produce enough
insulin, type 1 diabetes (previously known as
juvenile diabetes) occurs. Often occurs in people
who are less than 40 years old. - Symptoms include excessive
- - thirst, hunger, urination, and weight
loss. - In children and teens, the condition is usually
an autoimmune disorder in which specific immune
system cells and antibodies produced by the
immune system attack and destroy the cells of the
pancreas that produce insulin.
26
Diabetes Millitus
- The disease can cause long-term complications
including kidney problems, nerve damage,
blindness, and early coronary heart disease and
stroke. - To control blood sugar levels and reduce the risk
of developing diabetes complications, kids with
this condition need regular injections of insulin
27
Type I - DM
- Autoimmune disorder due to beta cell destruction
- Occurs in genetically susceptible individuals
(islet cell antibodies) - Typical onset is before the age of 30
- Can result in ketoacidosis (DKA).
28
Pathophysiology
- Type 1 DM is auto-immune mediated disease. The
bodys own T-Cell attack and destroy the
pancreatic beta cells which are the source of
insulin. In addition, autoantibodies to the islet
cells cause a reduction of 80 to 90 of normal
B cell before hyperglycemia and other
manifestations occur. - A genetic predisposition and exposure to virus
may contribute to the pathogenesis of Type 1 DM.
29
Pathophysiology
- Type 1 is associated with long preclinical
period. Islet cell antibodies responsible for
B-cell destruction are present for months to
years before onset of symptoms. - Manifestation develops when the persons pancreas
can no longer produce sufficient amount of
glucose to maintain normal glucose. Once this
occur, the onset of symptoms is usually rapid.
30
Type I - DM
- Clinical Characteristics
- serum glucose of 350 and above
- ketonuria in large amounts
- venous pH of 6.8 to 7.2
- serum bicarbonate below 15 mEq/dl
- 3 Ps
- Sudden weigh loss
- Without insulin, the cleint develops diabetic
ketoacidosis (DKA), a life threatening condition
resulting in metabolic acidosis.
31
Prediabetes
- It is a condition in which individuals are at
increased risk for developing diabetes. - Blood glucose are high but not high enough to
meet diagnostic criteria for DM. - Impaired Fasting Glucose (IFG) or Impaired
glucose tolerance (IGT). - Most people with prediabetes are at increased
risk for developing Type 2 DM, and if no
preventive measures are taken, they will usually
develop it within 10 years.
32
DM- Type 1 Collaborative Care and Treatment
- The goal of DM management is to reduce symptoms
and promote well-being, prevent acute
complications of hyperglycemia, and prevent or
delay the onset and progression of long term
complications. - Nutrition
- Drug therapy
- Exercise
- And self-monitoring of blood glucose are the
tools used in management of DM.
33
Drug Therapy
- The two major types of glucose lowering agents
(GLAs) used in treatment of DM are insulin and
oral hypoglycemic agents. - Insulin exogenous insulin is needed when a
client has inadequate insulin to meet specific
metabolic needs. - Type 1 requires insulin to survive.
- Type 2 requires insulin during period of severe
stress such as illness or surgery.
34
Insulin
- Insulin is prepared through the use of genetic
engineer ( derived from common bacteria (e.g. E.
Coli) or yeast cells using recombinant DNA
technology. - They differ in regards to onset, peak, and
duration. - Categorized as rapid acting, short-acting,
intermediate-acting, and long acting.
35
Drug Therapy Types of Insulin
Classification Example Clarity of Solution Characteristics
Rapid-Acting Insulin Humalog ( Lispro) Aspart (Novolog) Glulisine (Aapidra) Clear Onset less than 15 minutes. Peak 0.5 to 1.5 hr. Duration 2- 6 hr. Administer 5 to 15 min before meals
Short-Acting Insulin Regular (Humulin R, Novolin R, ReliOn R) Clear Onset 30 60 min. Peak 2 - 3 hr. Duration 3 10 hr. Administer 30 min before meals
Intermediate-Acting Insulin NPH ( Humulin N, Novolin N, ReliOn N) Cloudy Onset 2 - 4 hr. Peak 4 10 hr. Duration 10 - 18 hr.
Long Acting Insulin Glargine (Lantus) Detemir (Levemir) Clear Peak None Duration 24 hour acting
Combination Therapy NPH/Regular 70/30 (humulin 70/30, Novolin 70/30, ReliOn 70/30 NPH/Regular 50/50 Lispro protamine/lispro 50/50 (Humalog Mix Aspart protamine/aspart 70/30 (Novolog mix 70/30 Cloudy
36
insulin pump
insulin pen
37
Subcutaneous Injection Sites
38
Self-administration of insulin
- Rotate injection sites
- Inject at a 90 angle (45 if thin). do not
aspirate - When missing rapid or short with long acting
insulin draw up the shorter-acting insulin into
the syringe first and than the longer-acting
insulin (reduces the risk of introducing
longer-acting insulin into shorter-acting insulin
vial). - Observe client perform self-administration and
offer additional instruction as indicated.
39
Nursing Related to Insulin Therapy
- Proper administration assessment of clients
response to insulin therapy, and education of the
client regarding administration of insulin , and
adjustment to, and monitoring and reporting of
side effects of insulin. - Assess the client who is new to insulin and
evaluate ability to manage this therapy safely.
This include the ability to understand
interaction of isulin, diet, and activity, and to
be able to recognize and treat appropriately the
sysmptoms of hypoglycemia.
40
Nursing Related to Insulin Therapy
- The client and the caregiver must also be able to
prepare and inject the insulin ( see Table 49-5
Lewis et al., 2011 pg. 1226. Additional teaching
or resources is needed if client or caregiver
lacks the ability. - Follow-up assessment of the client ( e.g.
lipodystrophy, hypoglycemic episodes, and
handling of hypoglycemic episodes). - A review of the client record of urine and blood
glucose test is also important overall glycemic
control.
41
Type II
- Often due to the development of resistance to
endogenous insulin - Individuals with a family disposition,
individuals who are obese and over the age of 40 - obesity, physical inactivity, high triglycerides
(gt250 mg/dl), and hypertension are the hallmark
risk factors for the development of insulin
resistance.
42
Type II - DM
- Type 2 diabetes, the most common type, can start
when the body doesn't use insulin as it should.
If body can't keep up with the need for insulin,
the individual may need to take pills
(hypoglycemic agents). - Some individuals need both insulin and pills.
Along with meal planning and physical activity,
diabetes pills help people with type 2 diabetes
or gestational diabetes keep their blood glucose
levels on target. - Several kinds of pills are available. Each works
in a different way. Many people take two or three
kinds of pills. - Some people take combination pills. Combination
pills contain two kinds of diabetes medicine in
one tablet. Some people take pills and insulin.
43
Type II
- Clinical Characteristics (sign and symptoms)
- hyperglycemia
- plasma hyperosmolality
- dehydration
- changed mental status
- Treatment
- isotonic IV fluid replacement and careful
monitoring of potassium and glucose levels - intravenous insulin (not always necessary)
44
signs symptoms of glucose alteration
hypoglycemia ( 50 mg/dL) hyperglycemia (gt250 mg/dL)
cool, clammy skin hot, dry skin
diaphoresis absence of diaphoresis
anxiety, irritability, confusion, blurred vision alert to coma (varies)
hunger nausea, vomiting, abdominal pain (with ketoacidosis)
general weakness, seizures (severe hypoglycemia) rapid deep respirations (acetone/fruity odor due to ketones)
slurred speech blurred vision
weight loss hunger
weakness lethargy
syncope confusion
45
Oral Agents
- Sulfonylureas
- Biguinides
- Alpha-glucosidase inhibitors
- Thiazolidinediones
- Meglitindes
46
oral anti-diabetic medications
- administer as prescribed
- avoid alcohol with sulfonylurea agents
(disulfiram-like reaction) - monitor renal function (biguanides)
- monitor liver function (thiazolidinediones and
alpha-glucosidase inhibitors - women of childbearing age may need to take
additional contraception methods since the drugs
reduce the blood levels of some oral
contraceptives
47
Sick Day Management
- Illness and or infection can raise blood glucose
- the bodys response to illness and stress is to
produce glucose. any illness may result in
hyperglycemia - Patient teachings
- teach client to keep taking insulin or oral
anti-diabetic agents - monitor glucose more frequently (every 4 hours)
- watch for signs of hyperglycemia
- rest
48
Exercise
- regular, non-strenuous exercise
- exercise after mealtime
- exercise with a partner or let someone know where
the exercise will take place to ensure safety. - a snack may be needed before or during exercise
49
Diet
50
Diabetic Diet
- Type 1 Diabetes Diet - Type 1 diabetes always
requires insulin treatment, the main focus is to
find a balance between the food intake and
insulin. - Type 2 Diabetic Diet - Type 2 diet focus on
controlling weight in order to improve the body's
ability to utilize insulin. In most cases Type 2
diabetes can be controlled through proper diet
and exercise alone. - Gestational Diabetes Diet - unlike the Type 2
diet, gestational diabetes diet focus on adequate
energy and nutrients to support both the mothers
body and growing baby while maintaining stable
blood glucose levels for the pregnant mother.
51
Diabetic Diet
- Healthy eating helps to reduce blood sugar. It is
a critical part of managing diabetes, because
controlling blood sugar can prevent the
complications of diabetes. - Wise food choices are a foundation of diabetes
treatment. - Diabetes experts suggest meal plans that are
flexible and take lifestyle and other health
needs into account. - Healthy diabetic eating includes
- - Limiting sweets
- - Eating often
- - Being careful about when and how many
carbohydrates is being - eaten.
- Eating lots of whole-grain foods, fruits and
vegetables - Eating less fat
- Limiting your use of alcohol
52
Diabetic Diet Goal
- The diet goal is to eat a balanced, portion
controlled meal that will allow body to stay on
an even keel throughout the day as the components
of each meal hit the system. - Eating every two to three hours is best, five or
six small meals being recommended, and light
exercise after each meal will help kick start the
digestive system and prevent a spike in sugar
levels.
53
Diabetic Diet Sample Meal And Food
- One serving of protein (3 oz of chicken, lean
beef or fish) - One serving of bread (whole grain roll, tortilla
or ½ cup pasta) - One serving of dairy (cheese, milk or low-fat
sour cream) - One serving vegetables (fist sized portion or a
small bowl of salad) - One serving fruit (tennis ball sized or ½ cup
sliced) - Small amounts of unsaturated fats are needed, so
add a little dressing or a pat of soft margarine.
Avoid sweets consider the fruit your dessert! - Foods that should be avoided include fatty red
meat, organ meat, highly processed food, fried
food, fast food, high cholesterol food and foods
rich in saturated fat.
54
Diabetic Diet
- Generally Type 2 diabetic patients need 1500-1800
calorie diet per day to promote weight loss. - Calories requirement may vary depending upon
patients age, sex, activity level and body
weight. - Half of total daily required calories should
come from carbohydrates. - One gram of carbohydrate is about 4 calories. A
diabetic patient on a 1600 calorie diet should
get half of these calories from carbohydrate. In
other words it will be equal to 800 calories from
carbohydrates, it means they need 200gms of
carbohydrates everyday.
55
Improving The Sensitivity For Insulin
- When glucose balance is improved, the sensitivity
of all cells to the hormone insulin also
improves. - Very important because insulin is the hormone
which opens the doors in all cells to allow
glucose to enter, in order to supply fuel for the
production of energy. - Once this process is ineffective or out of
balance diabetic symptoms, signs of diabetes, pre
diabetes, or the cause of diabetes can occurs.
56
Hypoglycemia
- check blood glucose levels
- treat with 15 g carbohydrates
- recheck blood glucose in 15 minutes
- if still low, give 15 more g of carbs
- recheck blood in 15 minutes
- if normal, take 7 g of protein (if next meal is
more than an hour away)
?15 g of carbs (examples) 4 oz orange juice, 2
oz grape, 8 oz milk, glucose tablets ?7 g
protein (example) 1 oz string cheese fluid is
more readily absorbed (juice, non-diet drink,
skim milk
57
NANDA nursing diagnosis
- risk for injury
- imbalanced nutrition
- risk for impaired skin integrity
- deficient knowledge
- self-care deficit
- ineffective coping
58
- eye problems damage to blood vessels in the eyes
(retinopathy), pressure in the eye (glaucoma),
and clouding of the eye (cataract) - tooth and gum problems (periodental disease)
loss of teeth and bone - blood vessel (vascular) disease leading to
circulation problems, heart attack, or stroke - problems with sexual function
- kidney disease (nephropathy)
- nerve problems (neuropathy), causing pain or loss
of feeling in your feet and other parts of your
body - hight blood pressure (HTN), putting strain on
your heart and blood vessels - serious infections possibly leading to loss of
toes, feet or limbs
Complications
59
Diabetic retinopathy
- can cause blindness
- encourage yearly exams refer to opthalmologist.
- encourage management of glucose levels
- diet low fat, high in fruits, vegetables ad
whole grains - encourage a dietary consult
60
Foot care for the diabetic clients
- inspect feet daily and wash with mild soap and
warm water - pat feet gently especially between the toes
- use mild foot powder on sweaty feet
- do not use commercial remedies for calluses or
corns - consult a podiatrist
- cut toenails even with rounded contour of toes
- cut toe nails after a bath or shower
- separate overlapping toes with cotton or lambs
wool - do not go out barefoot
- wear clean absorbent socks
- do not use water bottles or heating pads to warm
feet. wear socks for warmth.
61
complications
diabetic foot ulcer
diabetic retinopathy
62
Diabetic Ketoacidosis DKA
Acute, life threatening condition characterized
by hyperglycemia (gt300 mg/dL) resulting in
breakdown of body fat for energy and an
accumulation of ketones on the blood and urine.
The onset is rapid, and the mortality rate of
DKA is 1 to 10
most common in individuals with type I diabetes
63
Diabetic Ketoacidosis
64
Diabetic Ketoacidosis
65
Hyperglycemic-Hyperosmolar Nonketonic Syndrome
(HHNS)
Acute life-threatening condition characterized by
profound hyperglycemia (gt600 mg/dL), dehydration,
and absence of ketosis. the onset it generally
over several day, and the mortality rate of HHNS
is up to 15 or more
more common in older adult clients and in
individuals with untreated or diagnosed type II
diabetes
66
Nursing management DKA/HHS
- Patient closely monitored
- Administration
- IV fluids
- Insulin therapy
- Electrolytes
- Assessment
- Renal status
- Cardiopulmonary status
- Level of consciousness
- Patient closely monitored
- Signs potassium imbalance
- Cardiac monitoring
- Vital signs
67
laboratory analysis
Diagnostic Procedure DKA HHNS
serum glucose levels gt300 mg/dL gt600 mg/dL
serum electrolytes ? sodium ?potassium Na increased due to water loss K initially low due to diuresis, may increase due to acidosis increased secondary to dehydration
serum renal studies ? BUN ?Creatinine increased secondary to dehydration increased secondary to dehydration
ketone levels ? serum ?urine present present absent absent
serum pH (ABG) metabolic acidosis with respiratory compensation (Kussmaul respirations) absence of acidosis
Recommended
CrystalGraphics Presentations





























