
Abstract - PowerPoint PPT Presentation
1 / 1
Title:
Abstract
Description:
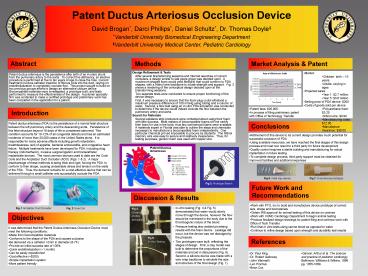
Patent Ductus Arteriosus Occlusion Device David Brogan*, Darci Phillips*, Daniel Schultz*, Dr. Thomas Doyle *Vanderbilt University Biomedical Engineering Department – PowerPoint PPT presentation
Number of Views:80
Avg rating:3.0/5.0
Title: Abstract
1
Abstract
Market Analysis Patent
- Market
- Children birth 15 years
- Adults varying in ages
- Projected sales
- Year 1 2.7 million
- Year 5 3.6 million
- Selling price of PDA device 200
- Costs of goods sold per device
- Polyurethane foam 3.25
- Nitinol wire 0.90
- Manufacturing costs 12.00
- Manufacture insurance 36.00
- Incremental cost 85.00
Design Refinement Tests After several
brainstorming sessions and Internet searches of
current occluders, a design similar to last years
group was decided upon. A mushroom shaped foam
would yield flexibility that could conform to PDA
shapes, with a Nitinol wire backbone to infuse
strength and support. Fig. 3 shows a rendering
of the conceptual design decided upon at the
brainstorming sessions. Two separate tests were
conducted to ensure proper functioning of the
device design. First, it was necessary to
ensure that the foam plug could withstand a
maximum pressure difference of 100 mmHg using
tubing and a column of water. Second, a flow
test using an in-vitro PDA simulation was
conducted to determine if the device would indeed
occlude the flow between the pulmonary artery and
aorta. Search for Materials Several epistaxis
strip producers were contacted about using their
foam, with little success. Most makers of
biocompatible foams will not certify their foam
for use in the body, thus few commercial foams
were available. A materials expert in Florida
was able to outline the steps and chemicals
necessary to manufacture a biocompatible foam
independently. One particular chemical proved
impossible to procure by students. The Nitinol
memory wire was easy to secure and relatively
inexpensive. Thus, for testing purposes, generic
foam was used with copper wire.
Patent ductus arteriosus is the persistence after
birth of an in-utero shunt from the pulmonary
artery to the aorta. To correct this deficiency,
an elective procedure is performed at five to ten
years of age to close the hole. Current treatment
involves catheter insertion of fibrous coils into
the duct, relying on endothelialization to
completely occlude flow. This project sought to
build on two previous groups efforts to design an
alternative closure device. Biocompatible
materials were investigated, a prototype built,
and tests performed to measure the effectiveness
of the design. A polymer specialty firm was
contacted to make a certified prototype and
preliminary work has been completed in the
application for a patent.
- Patent fees 20,000
- In process of filing preliminary patent with
Office of Technology Transfer
Patent ductus arteriosus (PDA) is the persistence
of a normal fetal structure between the left
pulmonary artery and the descending aorta.
Persistence of this fetal structure beyond 18
days of life is considered abnormal. This
condition accounts for 10-12 of all congenital
defects and has an estimated incidence of more
than 20,000 cases in the United States alone. It
is responsible for many adverse effects including
growth retardation, breathlessness, lack of
appetite, bacterial endocarditis, and congestive
heart failure. Multiple treatments have been
developed for PDA, including drug therapy
(indomethacin), invasive surgical ligation and
transcatheter implantable devices. The most
common devices used to date are the Cook Coils
and the Amplatzer Duct Occluder (ADO) (Figs. 1
2). A major disadvantage of these methods is
being thick and rigid, forcing the PDA to
conform to their shape, causing undesirable
stress and tension on the walls of the PDA.
Thus, the demand remains for a cost-effective
device that can be delivered through a small
catheter and successfully occlude the PDA.
- Refinement of this device to its current design
provides much potential for successful occlusion
of PDA - Using available resources, we have reached the
final stages of this design process and must now
resort to a third party for future development - Quality control requires a sterile building and
manufacturing for actual implantation in future
testing - To complete design process, third party support
must be obtained for improved facilities and
additional expenses
- Work with PTG, Inc to build and manufacture
device prototype of correct size, shape and
biomaterials - Obtain IRB approval for animal testing of this
device on canines - Work with VUMC Cardiology Department to begin
animal testing - Produce finalized design drawings for patent
filing and continue work with Office of Tech
Transfer - Run final in vitro tests using canine blood as
opposed to water - Continue to refine design based upon strength and
durability test results
- In-vitro testing (Fig. 4 Fig. 5) demonstrated
that water would slowly move through the device,
however the flow should be minimized in the body
due to the thrombogenic nature of the blood. - Pressure testing also yielded promising results
with the foam device. Leakage did occur, but the
device was not dislodged by the pressure. - Two prototypes were built, reflecting the stages
of design. First, a clay model was built to
determine the proportions of the materials and
aid in discussions (Fig. 6). Second, a silicone
device was made with a wire wrap backbone to
simulate the size and structure of the final
design (Fig. 7).
Fig 4. Close-up of PDA Simulation
- It was determined that the Patent Ductus
Arteriosus Occlusion Device must meet the
following conditions - Made from biocompatible materials
- Conforms to the shape of the PDA and causes
occlusion - Be delivered via a catheter lt2mm in diameter
(6-7F) - Provide an initial success rate of 100
- Quick endotheliazation (1 month)
- Can be easily repositioned
- Cost effective (lt200)
- Simple implantation system
- More patient friendly
Recommended
CrystalGraphics Presentations





























