
Identifying and Overcoming Barriers to Implementation of - PowerPoint PPT Presentation
1 / 1
Title:
Identifying and Overcoming Barriers to Implementation of
Description:
Identifying and Overcoming Barriers to Implementation of Shared Decision Making and Decision Aids Megan A. Morris, MS CCC-SLP 1,2; Anne D. Renz, MPH1; Douglas A ... – PowerPoint PPT presentation
Number of Views:63
Avg rating:3.0/5.0
Title: Identifying and Overcoming Barriers to Implementation of
1
Identifying and Overcoming Barriers to
Implementation of Shared Decision Making and
Decision Aids Megan A. Morris, MS CCC-SLP 1,2
Anne D. Renz, MPH1 Douglas A. Conrad, PhD, MBA,
MHA1 Carolyn A. Watts, PhD1 1 Dept. of Health
Services, University of Washington, Seattle,
Washington, USA 2 Dept. of Rehabilitation
Medicine, University of Washington, Seattle,
Washington, USA
Introduction and Background In 2007 the
Washington State Legislature passed a bill
mandating that the Health Care Authority (a state
agency) implement a shared decision making (SDM)
demonstration project at one or more
multi-specialty practice sites. Because the
legislation did not include appropriated funds,
the Health Care Authority sought collaborators
for the demonstration. Researchers from the
University of Washington obtained funding to
facilitate an SDM and decision aid (DA)
demonstration project. Three practice sites in
western Washington are currently participating in
the project. The demonstration project began in
2008. Early steps in the project included
obtaining IRB approval, identifying executive
champions and project managers at each site,
choosing conditions of interest, and creating
workflow process maps. Once this was
accomplished, the sites began to distribute DAs.
Multiple barriers, anticipated and unanticipated,
were identified at this stage of the project.
The following is a description of the identified
barriers and methods used to overcome those
barriers.
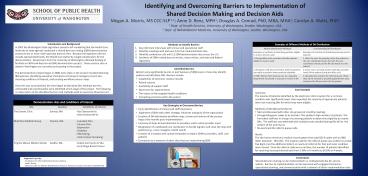
Examples of Different Methods of DA Distribution Examples of Different Methods of DA Distribution
Patient Identification Methods Corresponding DA Distribution
Examples of methods of identifying patients eligible to receive decision aids Examples of methods of distributing decision aids to patients
1. During office visits, providers identify patients eligible to receive a DA. 1. After the visit, the provider refers the patient to the care coordinator down the hall. The care coordinator introduces the DA and hands it to the patient.
2. Reception staff who are familiar with the patients can notify a provider about potential eligibility. 2. Exam rooms are kept stocked with DAs provider hands DA to patient during the office visit.
3. EPIC referrals from primary care to a specialty department are placed in a queue to receive a DA. 3. Receptionists monitor the referral queue. When they call to schedule a specialty appointment, they introduce the DA and mail it to the patient.
- Methods to Identify Barriers
- Key informant interviews with clinical and
operational staff - Monthly meetings with partners from the
implementation sites - Monthly conference calls with 11 SDM
demonstration sites across the U.S. - Synthesis of SDM-related journal articles, news
articles, and state and federal legislation
- Identified Barriers
- Barriers vary significantly by site, in part
because of differences in how sites identify
patients and distribute DAs. Barriers include - Capabilities of electronic medical records
- Patient volume
- Availability of support staff
- Wait times for appointments
- The nature of the targeted health conditions
- Competing priorities within the system
- Case Example
- Summary
- The volume of patients identified by the
electronic referral system for a common condition
was significantly lower than expected the
majority of appropriate patients were not
receiving DAs for which they were eligible. - Methods of Identifying the Barrier
- Met and discussed with other site groups (at
monthly meeting) - Changed diagnosis codes to be broader. This
yielded a high number of patients. The front desk
staff was in charge of screening patients to
determine eligibility to receive DAs. The staff
was overwhelmed with multiple tasks and
distributing DAs fell to the bottom of the
priority list. - Re-examined the referral queue code
- Result
- The site had an electronic medical record system
that used ICD-9 codes with an IMO letter
(example 784.15C). The original code for the
referral queue was written to accept five digits
(not the additional letter), so nearly all
referrals for that particular condition were
missed. Once the referral code was re-written,
the number of patients identified for receiving
increased dramatically from 3 DAs in 6 months to
26 DAs in 4 weeks.
Demonstration sites and conditions of interest Demonstration sites and conditions of interest Demonstration sites and conditions of interest
Site Location Conditions of Interest
The Everett Clinic Everett, WA - Hip Osteoarthritis - Knee Osteoarthritis
MultiCare Medical Group Tacoma, WA - Low Back Pain - Chronic Pain - Depression Diabetes PSA Testing Colon Cancer Screening
Virginia Mason Medical Center Seattle, WA - Ductal Carcinoma In Situ - Early Stage Breast Cancer
- Key Strategies to Overcome Barriers
- Early identification of clinical and staff
champions - Alignment of SDM with other strategic
initiatives and goals of the organization - Creation of DA distribution workflow maps review
and revision of the process maps a few
months post implementation - Inclusion of steps to feed data back to
providers and to solicit provider input - Designation of a dedicated care coordinator to
handle logistics and close the loop with patients
(e.g., nurse navigator, health coach) - Creation of a toolbox with sample templates to
explain SDM to providers, staff, and patients - Connection to a network of other sites that are
implementing SDM
Conclusions Shared decision making can be
implemented in a multispecialty fee-for-service
system. Barriers to implementation can be
overcome with engaged champions, operational
planning, and communication with a network of
other implementation sites.
- Supported in part by
- - Foundation for Informed Medical Decision Making
- Health Dialog
- National Center for Medical Rehabilitation
Research, National Institutes of Health
(T32HD007424)
Recommended
CrystalGraphics Presentations





























