
Burns - PowerPoint PPT Presentation
Title:
Burns
Description:
Burns constitute a major global problem and are a leading cause of trauma deaths ... layer which allows the skin to be loosely attached to the underlying fascia. ... – PowerPoint PPT presentation
Number of Views:136
Avg rating:3.0/5.0
Title: Burns
1
Burns
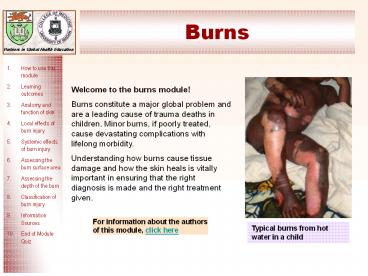
Welcome to the burns module! Burns constitute a
major global problem and are a leading cause of
trauma deaths in children. Minor burns, if poorly
treated, cause devastating complications with
lifelong morbidity. Understanding how burns cause
tissue damage and how the skin heals is vitally
important in ensuring that the right diagnosis is
made and the right treatment given.
For information about the authors of this module,
click here
Typical burns from hot water in a child
2
How to use this module
- This self - directed learning (SDL) module has
been designed for medical and other health care
students. - We suggest that you start with the learning
objectives and try to keep these in mind as you
go through the module slide by slide, in order
and at your own pace. - You should research any issues that you are
unsure about. Look in your textbooks, access the
on-line resources indicated at the end of the
module and discuss with your peers and teachers. - Finally, enjoy your learning! We hope that this
module will be enjoyable to study and complement
your learning about burns from other sources.
3
Learning outcomes
- By the end of the module, you should be able to
- describe the structure of the skin
- outline the local and systemic effects of burn
injury - assess the size of burns accurately
- assess the depth of burns accurately and relate
how this determines the way in which it heals - classify burn injuries according to the type of
treatment required (outpatient, inpatient or
specialist care)
4
Anatomy of skin (1)
Epidermis
basement membrane
Dermis
Subcutaneous layer
The skin is made up of two layers, the outer
layer (epidermis) and inner layer (dermis).
Between the epidermis and dermis is the basement
membrane which is semi permeable and acellular.
It provides support, flexibility and regulates
the transfer of substances across the
dermal-epidermal junction. Under the skin is the
subcutaneous layer which allows the skin to be
loosely attached to the underlying fascia. It
increases mobility and is especially important
over joints.
5
Anatomy of skin (2)
Thickness of skin increases from birth until
approximately 40 years of age, then it starts to
thin again. It also varies over different parts
of the body.
- Which of the following areas do you think has a
thin epidermis? - Eyelid
- Palm
- Foot
Click to Reveal Answers
The eyelid has a thin epidermis (0.05mm). The
palm and foot have a thick epidermis (gt1.5mm).
6
Anatomy of skin Epidermis (1)
- A protective barrier of stratified
- squamous epithelium consisting of 5
- layers
- Stratum corneum 20-30 rows of dead cells
continually shed - Stratum lucidum 3-4 layers clear flat dead cells
- Stratum granulosum Cells degenerating with
production of keratin - Stratum spinosum 8-10 rows of cells that produce
protein but can not duplicate - Stratum basale Columnar cells continually
dividing, gradually migrating to surface
EPIDERMIS
There are three other cell types within the
epidermis melanocyte, Langerhan and Merkel cells
7
Anatomy of skin Epidermis (2)
- Other cell types within the epidermis
- Melanocytes Produce melanin pigment causing
brown colouration of skin and protects skin from
UV light damage - Langerhan cells Immune cells which help in
defence. Situated in stratum spinosum, they help
process and present foreign antigens to the
immune system - Merkel cells Within the basal layer, close to
hair follicles involved in touch sensation
Click to Reveal Answers
None of them! All racial groups have the same
number of melanocytes, but dark skin individuals
have more metabolically active cells which
produce more melanin.
(a) (b) (c)
Who do you think has more melanocytes (a), (b) or
(c)?
8
Anatomy of skin Dermis (1)
- The dermis consists of 2 layers
- Papiliary dermis The upper layer of dermis. It
has extensions protruding into the epidermis
called Rete pegs which also contain small
capillary loops - Reticular dermis The lower layer of dermis. It
is made up of collagen, elastin and ground
substance as well as hair follicles, sweat and
sebaceous glands - Fibroblasts are the predominant cell type in the
dermis and produce collagen and elastin which
provide strength and flexibility to the skin. - In addition, there are blood vessels, sebaceous
glands, sweat glands, hair follicles, sensory
receptors and fat cells.
9
Anatomy of skin Dermis (2)
- There are other cell types and structures within
the dermis - Myofibroblasts - contractile, important in
healing of wounds - Macrophages - derived from vascular leucocytes
phagocytic and stimulate fibroblasts - Mast cells - contain histamine
- Lymphocytes - mediate immune function
- Sensory receptors
- Meisners Khause Ruffins Paccinian
- Texture Cold Heat Vibration deep
pressure
10
Functions of the skin
Physical barrier
Vitamin D production
Immunity
Sensation
Identity
Temperature control
Remember P V I S I T !
11
Local effects of burn injury (1)
- Summary of local effects
- Cell death/disturbed function
- Release of inflammatory mediators
- Increased capillary permeability
- Microvascular thrombosis
- 1. Cell death/disturbed function
- Cellular function is disturbed when the
temperature rises above 43oC. The higher the
temperature and more prolonged the contact, the
more cells die. An instantaneous full thickness
burn occurs at a temperature of 700C or greater.
Due to differences in skin thickness with age, at
55?C, severe damage occurs after 10 seconds in a
child and 30 seconds in an adult. Skin thickness
is also reduced in older people and in certain
conditions (e.g. steroid therapy).
12
Local effects of burn injury (2)
- 2. Release of inflammatory mediators
- Potent vasoactive mediators are released from the
burn wound. These include - vasoconstrictors and vasodilators, histamine,
serotonin, kinins, prostaglandins - and oxygen free radicals
- Thromboxane causes platelet aggregation and
microvascular thrombus formation - Histamine released by mast cells causes
increase in capillary permeability - Prostaglandins result in arteriolar dilatation
- Kinins increases vascular permeability
- Serotonin increases vascular resistance and
venous hydrostatic pressure leading to oedema - Oxygen free radicals increase vascular
permeability
13
Local effects of burn injury (3)
- 3. Increased capillary permeabilityWhen
capillaries are damaged, they leak protein-rich
fluid which results in oedema.
Normal skin normal capillary permeability
Burn wound oedema with increased capillary
permeability and protein leakage
14
Local effects of burn injury (4)
- 4. Microvascular ThrombosisRelease of
thrombogenic factors such as thromboxane,
together with a hypovolaemic state cause sludging
in the smallest blood vessels. This in turn leads
to further tissue ischaemia, increased cell death
and can cause extension of the depth and surface
area of the burn.
Area of burn increases due to sludging in blood
vessels and ischaemia
15
Systemic effects of burn injury (1)
- When a burn is large (gt20 of total body surface
area), in addition to the local response, there
is also a systemic response - Vasoactive substances are released that act not
just locally in the burned tissue, but in
non-burned tissue as well.
Loss of circulating blood
With large burns, the loss of circulating blood
volume will rapidly lead to HYPOVOLAEMIC SHOCK,
unless resuscitation is started
Ischaemia
Vascular permeability
16
Systemic effects of burn injury (2)
Click each box
Psychological system
Respiratory system
Cardiovascular system
Immune system
Renal system
Gastrointestinal system
Haematological system
17
Systemic effects of burn injury psychological
system
- Psychological Effects
- 1. Post traumatic stress disorders
- 2. Mood and anxiety disorders
- 3. Depression especially with facial
disfigurement - Social problems such as difficulty in sexual
relations and social interactions
Back
18
Systemic effects of burn injury respiratory
system
Respiratory system
- Thermal injury to upper airway may result in
mucosal swelling and obstruction - Inhalation injury to lower airways may result in
progressive pulmonary failure from
ventilation-perfusion mismatch - Beware over aggressive fluid resuscitation can
cause or exacerbate pulmonary oedema especially
in infants
Back
19
Systemic effects of burn injury cardiovascular
system
Cardiovascular system
Circulating volume Venous return Cardiac
output Peripheral vascular resistance
Back
20
Systemic effects of burn injury immune system
Immune system
- Initial inflammatory phase
- increased circulating immunoglobulins
- activation of complement system
- elevated acute phase proteins
- Immune suppression phase
- decreased circulating immunoglobulins
Back
21
Systemic effects of burn injury renal system
Renal system
- (1) Renal blood flow Glomerular filtration
rate - ADH production Aldosterone
- Na H20 retention
-
? generalised oedema - Tubular dysfunction ( acute tubular necrosis)
- Beware high-voltage electrical injury may be
complicated by rhabdomyolysis and myoglobinuria
Insert image of nephron
Back
22
Systemic effects of burn injury
gastrointestinal system
Gastrointestinal system
- Ulceration (stress ulcers)
- Ileus
- Bacterial translocation
- Cholestasis
- Liver dysfunction (deranged enzymes, decreased
synthesis of clotting factors and proteins)
Back
23
Systemic effects of burn injury haematological
system
Haematological system
- Anaemia, caused by
- ? half life of red blood cells
- haemolysis
- Neutrophilia
- Thrombocytopaenia
Back
24
Assessing total burn surface area (TBSA)
Click to Reveal Answers
- The area of this burn is about 3-5 of total body
surface area.
How much of the body surface area is burnt?
- There are several ways to assess the size of a
burn. They all consider the burnt area as a
percentage of the total body surface area and are
supported by mapping the burnt area on a diagram.
In the next couple of slides, we will be looking
at the following methods of assessment - The rule of 9s
- Lund and Browder charts
- Palm of hand
- Unburnt area
25
Assessing TBSA - Rule of Nines
- This method divides the body into areas each of
which equates to 9 of the total body surface
area - the whole of one arm (anterior and posterior
surfaces including the hand) is 9, therefore 2
arms 18 - the entire head including face, scalp and neck
is 9 - anterior trunk is 18
- posterior trunk including buttocks is 18
- the whole lower limb (anterior and posterior
surfaces, including the thigh, leg and foot) is
18 therefore both lower limbs 36. - This totals 99 with the perineum making the
final 1. - Beware this method is unreliable in young
children.
26
Assessing TBSA in children
Why might the rule of 9s be unreliable in
children?
Click to Reveal Answers
Body proportions change with age. In a child, the
head represents a much greater proportion of the
total body surface area.
27
Assessing TBSA - Lund and Browder charts
These take account of the patients age and
provide a more detailed mapping system for the
burnt area
AREA AGE 0 1 5 10 15 ADULT
A ½ OF HEAD 9 ½ 8 ½ 6 ½ 5 ½ 4 ½ 3 ½
B ½ OF ONE THIGH 2 ¾ 3 ¼ 4 4 ½ 4 ½ 4 ¾
C ½ OF ONE LEG 2 ½ 2 ½ 2 ¾ 3 3 ¼ 3 ½
28
Assessing TBSA - Palm size
- Another useful way, especially for small burns is
to use the palm of the patients hand (with
fingers extended). This equates to approximately
1 of the body surface area.
29
Assessing TBSA - Unburnt area
- In very large burns, it is often easier to
measure the area of skin that is unburnt and then
subtract this from 100.
30
Area of the body involved
Not only is the surface area or size of burn
important, but also the specific part of the body
affected
Eyes Burns to the eyes (especially chemical)
can cause blindness.
Face Facial oedema can lead to airway
obstruction. Scarring can cause significant
psychosocial problems
Feet Mobility problems
Hands Problems with feeding and hygiene
Perineum problems with urogenital function and
psychosexual
Circumferential burns of the limbs can cause
distal ischaemia of the chest, can compromise
breathing
31
Depth of burn
- The depth of a burn determines its treatment and
how long it takes to heal. - For this reason, it is important to be able to
assess the depth as - Superficial
- Partial thickness
- Superficial partial thickness
- Deep partial thickness
- Full thickness
32
Depth of burn - Superficial (erythema)
- Involves epidermis only
- Painful
- Red
- No blistering
- Heals rapidly (reversible injury)
- No permanent scars
- Note that erythema is NOT included when assessing
TBSA
33
Depth of Burn superficial partial thickness
Typical hot water scald
- Involves epidermis and upper dermis
- Red
- Blistering, moist
- Painful
- Heals by epithelialization
- Healing complete within 14 days
- Minimal or no permanent scars
- but can leave discolouration
Glistening moist red/pink appearance typical of
superficial injury
Patches of skin that would come off on cleaning
34
Depth of Burn - superficial partial thickness
Pin-point bleeding
Pink surface blanches on pressure
Blister
35
Depth of Burn deep partial thickness
- Involves epidermis, upper dermis and varying
degrees of lower dermis - Pale, mottled appearance
- Fixed staining (no blanching)
- May be painful or insensate (depending on depth)
- Heals by combination of epithilialization and
wound contracture - May take weeks to heal
- Can leave significant scars and contractures over
joints depending on time taken to heal
Deep dermal area, reddish with fixed staining
36
Depth of Burn full thickness
- Involves all of epidermis and all of dermis
- Dry, leathery (white, dark brown or charred)
- Insensate
- Heals by contraction
- Delayed healing
- Hypertrophic or keloid scars
- Leads to contractures
Dry, leathery, charred appearance of a full
thickness burn
37
Circumferential full thickness burn
Black, charred skin
Typical position of hand in full thickness burns
with metacarpophalangeal joints extended and
interphalangeal joints flexed
38
Depth of Burn mixed thickness
Assess the depth of the burn in areas A, B and C
Click to Reveal Answers
39
Depth of Burn Mixed thickness
Full thickness, dry white leathery appearance
Deep dermal with pale pink and white patches, non
blanching
Superficial partial thickness showing pink
blanching
40
Classifying the patient
- First you should assess the severity of the burn
injury according to - TBSA
- depth
- position
- presence of infection
- time since the burn
- presence or absence of inhalation injury
- Combine this information with patient factors
- age
- associated injuries
- other medical problems
- nutritional status
- Finally consider social and family factors to
classify the patient according to how and where
to provide treatment.
41
A guideline for patient classification
Factors
Burn injury
Large
Moderate
- TBSA
Small
Full thickness
Partial thickness
- depth
Superficial
Critical area
Non-critical area
- position
- presence of infection
Systemic
Localised
Absent
severe
mild
Absent
- inhalation injury
Patient factors
Extremes of age
Adult or older child
- age
significant
none
- associated injuries
significant
none
- other medical problems
- nutritional status
Malnourished
Normal
Social / family factors
Unable to care for oneself
Able to care for oneself
Specialist
In-patient
Out-patient
42
Authors and reviewers
- Authors
- Welsh Centre for Burns and Plastic Surgery, UK
- Tom Potokar Consultant Plastic Surgeon
- Prakash Lohana SHO in Plastic Surgery
- College of Medicine, University of Ibadan,
Ibadan, Nigeria - Abiodun Alao Senior System Analyst
- Kemi Tongo Lecturer and Consultant paediatrician
- The School of Medicine, Swansea University,
Swansea, UK - David Lewis Learning Technologist
- Stephen Allen Reader in Paediatrics and Honorary
Consultant Paediatrician
We are very interested to receive feedback
regarding any aspect of this module especially
if it helps us to improve it as a learning
resource. Please e mail any comments to
Tom.Potokar_at_swansea-tr.wales.nhs.uk For further
information about the Partnership in Global
Health Education, visit http//www.medicine.swan.
ac.uk/inthealth.html
Back
43
Sources of information
- Some images have been adapted from CorelDraw
clipart - See www.interburns.org for more information
44
End of Module Quiz
Well done! Now that you have completed the burns
module you may wish to try these questions to
assess your learning. First, print-out the
questions and write down your answers to each
one. Then look at the answer sheet to assess
your learning.
Questions
Answers
Recommended
CrystalGraphics Presentations





























