
3. MALIGNANT MELANOMA - PowerPoint PPT Presentation
1 / 27
Title: 3. MALIGNANT MELANOMA
1
3. MALIGNANT MELANOMA
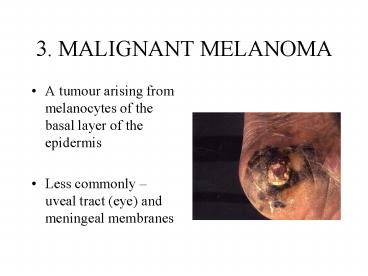
- A tumour arising from melanocytes of the basal
layer of the epidermis - Less commonly uveal tract (eye) and meningeal
membranes
2
INCIDENCE
- Global incidence is rising relentlessly
- In NI, the incidence rate of melanoma is
increasing faster than any other tumour - 1996 181 new cases of malignant melanoma
- On average 28 deaths due to melanoma each year
3
RISK FACTORS FOR MELANOMA
- Large numbers of benign naevi
- Freckles
- Clinically atypical naevi
- Severe sunburn
- Early years in a tropical climate
- Family history of MM
4
(No Transcript)
5
PATIENT EDUCATION
6
FAMILY HISTORY
- The majority of MMs occur in a sporadic pattern
- 2-10 of patients presenting with MM give a
positive family history - In part this may be due to the inheritance of
specific MM susceptibility genes eg, CDKN2A on
chromosome 9 - Other reasons for familial clustering are
atypical naevi and sun exposure
7
NAEVI
- CONGENITAL NEVI occur in 1 of newborns. Tend
to be large. Increased risk of MM - ACQUIRED MELANOCYTIC NAEVI 30-50 of all MMs
arise in pre-existing naevi. ?nos of naevi?risk
MM - ATYPICAL NAEVI / SYNDROME association between a
familial occurrence of MM and an atypical naevus
phenotype
8
SUNSCREENS
- Have been promoted as protective agents
- But this is not supported by epidemiological data
- ? Causal role of sunscreen chemicals
- ? False sense of security in those at risk
spend longer out doors but dont reapply
appropriately
9
AIDS IN CLINICAL DIAGNOSIS
- GLASGOW SYSTEM
- Major
- Change in size
- Irregular pigment
- Irregular outline
- Minor
- Diameter gt6mm
- Inflammation
- Oozing/bleeding
- Itch/altered sensation
- AMERICAN ABCDE
- SYSTEM
- Asymmetry
- Border
- Colour
- Diameter
- Examination
10
TYPES OF MELANOMA
11
NODULAR
- Commoner in males
- Trunk is a common site
- Usually thick with a poor prognosis
- Black/brown nodule
- Ulceration and bleeding are common
12
SUPERFICIAL SPREADING
- The most common type of MM in the white-skinned
population 70 of cases - Commonest sites lower leg in females and back
in males - In early stages may be small, then growth becomes
irregular
13
ACRAL LENTIGINOUS MELANOMA
- In white-skinned population this accounts for 10
of MMs, but is the commonest MM in
nonwhite-skinned nations - Usually comprises a flat lentiginous area with an
invasive nodular component
14
SUBUNGAL MELANOMA
- Rare
- Often diagnosed late confusion with benign
subungal naevus, paronychial infections, trauma - Hutchinsons sign spillage of pigment onto the
surrounding nailfold
15
LENTIGO MALIGNA MELANOMA
- Occurs as a late development in a lentigo maligna
- Mainly on the face in elderly patients
- May be many years before an invasive nodule
develops
16
AMELANOTIC MELANOMA
- Diagnosis is often missed clinically
- The lack of pigmentation is due to the rapid
growth of the tumour and the differentiation of
the malignant melanocytes
17
METASTATIC MELANOMA
18
PROGNOSTIC VARIABLES
- The Breslow thickness is the single most
important prognostic variable (distance in mm of
the furthest tumour cell from the basal layer of
the epidermis)
19
- Scalp lesions worse prognosis, then palms and
soles, then trunk, then extremeties - Younger women appear to do better than either men
at any stage or women over 50 - Ulceration of the tumour surface is a high risk
factor
20
MANAGEMENT
- Surgical excision 1-3cm margins depending on
breslow depth - Invasive primary MM on the digits can be treated
by amputation - Need to investigate all MMs over 1mm for
metastases CXR, USS abd or CT chest, abd,
pelvis, bloods FBP, LFTs, LDH - New scanning modality in Belfast PET scan for
high risk primaries or evaluating lymphadenopathy
21
(No Transcript)
22
FOLLOW UP
- No general agreement on time period
- Depends on tumour thickness
- Thick tumours 5-10 years
- Need to examine the scar and check for
lymphadenopathy, liver, spleen, and total body
examination for other suspicious naevi
23
PLANTAR MALIGNANT MELANOMA
- Caucasians 1-9
- Asians 29-46
- Afro-Carribean 60-70
24
SUBUNGAL MELANOMA
TRAUMA
25
Dwyer PK et al British Journal of Dermatology
1993128115-120
- 51 white caucasian patients west of Scotland with
plantar melanoma - 20 sup spreading melanoma
- 27 acral lentiginous
- 4 nodular
- Femalemale 32
26
Franke W et al Melanoma Research 200010571-576
- Prognosis for plantar melanoma poor
- Poor survival can be improved by a significant
reduction in the time period between the first
observation of a plantar skin lesion and surgical
treatment
27
Walsh SM et al The Journal of Foot and Ankle
Surgery 200342(4)193-198
- ..that the clinician must maintain a high index
of suspicion when a patient presents with a
pigmented or atypical lesion on the foot.
Recommended
CrystalGraphics Presentations





























