
Management of BBS - PowerPoint PPT Presentation
1 / 9
Title:
Management of BBS
Description:
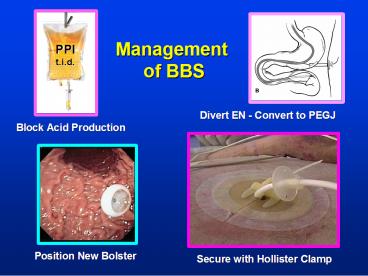
Management. of BBS. Position New Bolster. Divert EN - Convert to PEGJ. Secure with Hollister Clamp ... Correct Tension of PEG External Bolster. Communication ... – PowerPoint PPT presentation
Number of Views:202
Avg rating:3.0/5.0
Title: Management of BBS
1
Management of BBS
PPI t.i.d.
Divert EN - Convert to PEGJ
Block Acid Production
Position New Bolster
Secure with Hollister Clamp
2
Leakage and Peritonitis
3
Concern for Leakage and Peritonitis
Surgical Perspective
4
Correct Tension of PEG External Bolster
Communication with Endoscopist
8
6
External bolster
- Chung Study
- Tract Complicat
- Tight 4.9cm 13/48
- Loose 11.6cm 1/67
- Conclusion
- Firm for first 3-4 days
- Loose (1cm) thereafter
(gauze)
4
Abdominal wall
2
Gastric wall
Amer Surg 199056134
5
Excess Drainage Mass, Abscess, Breakdown
Passage of PEG Tube through Liver
6
Breakdown / NodularityMetastatic Seeding
- Rare, but 30 cases reported
- Aver time to dx 7.3-8.0 mos
- Sx Drainage Fungating mass
- Bleeding Superinfection
- May require local XRT vs surg
Pickhardt (AJR 2002179735) Brown (Am J Gasro 20
00953288)
7
Stool Around PEG Site Gastrocolocutaneous Fistula
I could swear that smells like
- Acute Peritonitis, infection, fasciitis,
obstruction - Chronic Stool at site, insidious diarrhea, at
tube removal
8
Stool Around PEG Site Gastrocolocutaneous Fistula
Mechanism
Inadvertant Puncture versus Delayed Erosion
9
Looking Out for Our Patients
- Nutrition Support Specialist Proactive in
longterm surveillance - Routine monitoring Reduce risk factors, early
identification - Simple techniques, good communication provide
prompt correction
Recommended
CrystalGraphics Presentations





























