
Emerging Complications: Diabetic Retinopathy - PowerPoint PPT Presentation
1 / 21
Title:
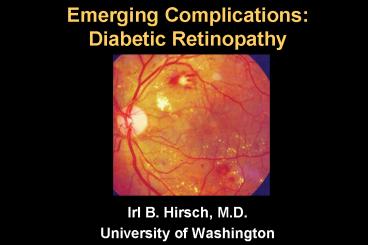
Emerging Complications: Diabetic Retinopathy
Description:
Emerging Complications: Diabetic Retinopathy Irl B. Hirsch, M.D. University of Washington Natural History 657 type 1 patients diagnosed between 1950 and 1980 with ... – PowerPoint PPT presentation
Number of Views:265
Avg rating:3.0/5.0
Title: Emerging Complications: Diabetic Retinopathy
1
Emerging ComplicationsDiabetic Retinopathy
- Irl B. Hirsch, M.D.
- University of Washington
2
Natural History
Pittsburgh Epidemiology of Diabetes
Complications Study
- 657 type 1 patients diagnosed between 1950 and
1980 with mean duration of 20 years - NPDR universal after 20 years duration
- PDR present in 70 after 30 years duration
- With shorter durations, PDR more prevalent in
females
Orchard TJ et al Diabetes 1990391116-24
3
Natural History
Pittsburgh Epidemiology of Diabetes
Complications Study
- The prevalence of retinopathy and overt
nephropathy in 552 White T1 subjects mean DM
duration 20.8 yr was significantly greater in
subjects diagnosed during puberty compared with
those diagnosed before puberty.
Kolstraba JN et al Diabetes Care. 198912686-9
4
Natural History
Pittsburgh Epidemiology of Diabetes
Complications Study
- Results concerning the risk of diabetes-related
mortality in a cohort of 1582 subjects (mean
duration 12.9 yr) indicated that postpubertal
duration of T1DM may be a more accurate
determinant of the development of microvascular
complications and diabetes-related mortality than
total duration, and it is suggested that the
contribution of the prepubertal years of diabetes
to long-term prognosis may be minimal.
Kolstraba JN et al Diabetes Care. 198912686-9
5
Major Question RE PDR and T1DM
When does the clock start ticking?
Does pre-pubertal status protect against DR? How
does puberty impact duration of diabetes for
teens and young adults?
6
German Registry Study
University of Ulm
- N441, median age 15.5 years, median duration
DM 6.3 years - 19 BID NPH/REG 42 TID injections, 40 QID
injections - Shortest duration prior to Dx of NPDR was 2.2
years - Youngest child with NPDR 5.5 years old
Holl RW, et al J Pediatr 199813279--794
7
German Registry Study
- Life table analysis revealed a median duration of
16.6 years until the occurrence of early DR
Holl RW, et al J Pediatr 199813279--794
8
German Registry Study
Pubertal Duration
- Comparing children with onset before to
during/after puberty, those with pre-pubertal Dx
developed DR a median of 10.9 years after puberty
compared to 15.1 years with pubertal onset of DM
Holl RW, et al J Pediatr 199813279--794
9
German Registry Study
- Good glycemic control (A1C lt 7.5) delayed the
onset of DR by about 3 years
NOTE DR was generally not prevented by good
control
Holl RW, et al J Pediatr 199813279--794
10
German Registry Study
- Pre-pubertal glycemic exposure does not protect
against DR - Metabolic control should be attempted
irrespective of age
Holl RW, et al J Pediatr 199813279--794
11
Ophthalmology 19931001125-31
12
Missouri DR Data
- N420 with onset lt 20 years of age enrolled
between 1979 and 1988 - Annual stereo fundus photographs
- Results
- No DR before 2 years in anyone
- 50 by 9 years DM duration
- 100 by 20 years duration
- DR developed 2 years sooner in females, but no
difference when considering pubertal status
13
(No Transcript)
14
Missouri PDR Data
- PDR developed in 11 patients
- Higher A1C with PDR (10.9 vs. 8.6)
- The higher the A1C, the sooner PDR detected
15
Missouri DR Data Conclusions
- Long-term glycemic control impacts both the
appearance and the progression of DR - Prepubertal duration of diabetes is a significant
risk factor for the development of DR
16
What About Screening of DR in Youth
- 667 children and adolescents at the Childrens
Hospital at Westmead, Sydney Australia - DR in lt 11 years old
- 16 baseline 1-2 years later, regressed in 80,
progressed in none - DR in gt 11 year olds
- 22 baseline 1-2 years later, regressed in 36,
progressed in 13
17
Screening of DR in Diabetic Youth
Risk of DR progression in children lt 11 years of
age
Maguire A et al. Diabetes Care 200528 509-13
18
Screening of DR in Diabetic Youth
Risk of DR progression in children gt 11 years of
age
Maguire A et al. Diabetes Care 200528 509-13
19
Screening of DR in Diabetic Youth
- In the highest risk group (gt 10 years duration DM
with A1C at any screening gt 10) DR progressed
significantly after 2 years but not until after 3
years in the group whose A1C was always lt 10 - Although patients with diabetes gt 10 years were lt
likely to have an improvement of their DR after 1
year, there was no increase in DR at 1 year
follow-up
Maguire A et al. Diabetes Care 200528 509-13
20
Screening of DR in Diabetic Youth
- These studies suggest that adolescents in
reasonable metabolic control could safely be
screened every 2 years instead of the current
yearly recommendation - In younger children the next screening could be gt
2 years later - Those with poor control (A1C gt 10), duration gt
10 years, or significant DR should be screened
more frequently
Maguire A et al. Diabetes Care 200528 509-13
21
Current ADA Recommendations
- 1. Adults and children aged 10 years or older
with type 1 diabetes should have an initial
dilated and comprehensive eye examination by an
ophthalmologist or optometrist within 5 years
after the onset of diabetes. (B) - 2. Subsequent examinations for type 1 and type 2
diabetic patients should be repeated annually by
an ophthalmologist or optometrist. Less frequent
exams (every 23 years) may be considered
following one or more normal eye exams.
Examinations will be required more frequently if
retinopathy is progressing. (B)
Diabetes Care 33 (Suppl 1) S11-61, 2010
Recommended
CrystalGraphics Presentations





























