
Echocardiographic evaluation of the - PowerPoint PPT Presentation
1 / 59
Title:
Echocardiographic evaluation of the
Description:
Title: Slide 1 Author: LIB2 Last modified by: DRAZARFARIN Created Date: 10/28/2006 4:29:26 AM Document presentation format: On-screen Show (4:3) Other titles – PowerPoint PPT presentation
Number of Views:216
Avg rating:3.0/5.0
Title: Echocardiographic evaluation of the
1
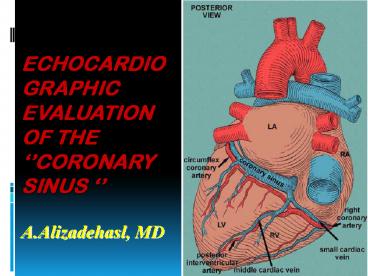
Echocardiographic evaluation of the coronary
sinus A.Alizadehasl, MD
2
(No Transcript)
3
(No Transcript)
4
Sub-Ao stenosis LSVC
5
Diastolic anterior motion of CS during rapid
ventricular filling and atrial systole
6
COA and LSVC draining to the CS
7
?
8
TAPVC to the CS
9
ASD2 LSVC
10
TF LSVC
11
(No Transcript)
12
(No Transcript)
13
(No Transcript)
14
- 31 adult pts free of significant
- coexisting disease and undergoing CABG.
- We measured CSBF velocity by using TEE and
hemodynamic variables, before and after CPB.
15
- After induction of anesthesia, by a 5-MHz
bi-plane TEE probe (Hewlett-Packard, Andover, MA
monitoring was conducted during anesthesia. By
using B-mode echo, we obtained a view of the CS
in the modified 4-C view.
16
(No Transcript)
17
- The pulse-Doppler sample volume was placed in the
CS 1 cm before its inflow in the RA. - The transducer position was optimized to obtain
an angle of 40 between the Doppler beam.
18
- We obtained a complete set of control
measurements and a complete set of post-CPB
measurements in 28 patients (90).
19
(No Transcript)
20
In the normal group, peak velocity, and VTI of
CSBF in the post-CPB period increased
significantly compared with the pre-CPB period
with CABG .
21
- We found that the peak velocity and VTI of CSBF
did not increase in the post-CPB period in the
new RWMA group despite the same changes of HR and
Hct in each group.
22
(No Transcript)
23
- There are several factors including
- Unsuccessful revascularization
- 2) Successful revascularization, but reperfusion
injury, stunning, hibernation in the immediate
post-CPB period - 3) Surgical trauma and myocardial damage or
infarction resulting in regional and/or global
blood flow decrease.
24
- The results of this preliminary study show the
feasibility of clinical evaluation of CABG
intraoperatively.
25
Measurment of coronary sinus blood flow after
first anterior myocardial infarction with
transthoracic echocardiography and study of its
association with wall motion scoring index
26
BACKGROUNDCSBF is often used as a measure of
cardiac perfusion. The standard techniques for
measurement are invasive and require cardiac
catheterization (intravascular Doppler flow wire,
thermodilution catheter,or digital coronary
angiography) or the use of radioisotope dyes
(argon technique or xenon scintigraphy).
27
AIMThe aim of this study is measuring of CSBF
and Cs.VTI via TTE in pts with AMI in association
with LVEF ,WMSI and in hospital mortality.
28
- METHODS
- In this cohort study 40 pts with ant.MI and 40
healthy individuals as controls, studied in 6
mounth period all of pts received routin AMI
treatment (e.g fibrinolytic). CSBF,Cs.VTI ,WMSI
and TDI data were obtained via TTE and compared
between the 2 groups.
29
A RV 2-chamber TTE was performed with a 2.5-MHZ
transducer to visualize the CS, and CFD was done
to confirm the flow within it. CSBF was
identified by PW recordings as systolic and
diastolic signals with very little respiratory
variation (in contrast to IVC flow).
30
- Baseline variables (AGESEXDMHTNHLP SMOKING
even BMI )were similar between 2 groups, all
p.values were gt 0.05.
31
(No Transcript)
32
(No Transcript)
33
Diameters of the CS taken at 5 equally spaced
segments in the cardiac cycle, over 3 cardiac
cycles, were averaged and used as the major
diameter of the coronary sinus. Assuming that the
cross section of the CS is an ellipse and that
the major diameter is double the length of the
minor diameter, the CSA of the CS was calculated
as 0.39 (the major diameter)2. CSBF was then
calculated as (VTI of the CS) (CSA of the CS)
(heart rate) .
34
Table1.Comparison of parameters between 2 groups.
CSBF AMI group. 287.8-/128ml/min Cs.VTI 11.16-/2.85cm
Control group. 415-/127ml/min P0.003 17.56-/2.72cm P0.001
35
- There was significant correlation between CSBF
and LVEF(r0.48,p0.002), WMSI (r-0.65,p0.002)
and in hospital MORTALITY - (r0.68,p0.03).
- -
36
- Also there was significant correlation between
Cs.VTI and LVEF (r0.84,p0.0001), WMSI
(r-0.77,p0.001)and in hospital MORTALITY rate
(r0.69,p0.02).
37
- CSBF and Cs.VTI had good correlation with TDI
findings(Sm septal).
38
- Our study demonstrated that CSBF and Cs.VTI were
INDEPENDENT predictors in AMI pts.
39
We concluded of significant decrease of CSBF (
303-/126 ml/min vs. 268-/121 ml/min p0.001)
and CSVTI ( 14.45-/2.85 ml vs.11.19-/2.69 ml
p0.003) in the pts with fragmented QRS in
comparison to the Acute Ant.MI pts without
fragmented QRS (especially accompanied by RBBB
CSBF 243-/118 ml/min and CSVTI 9.6-/2.34 ml )
while there was no differences in LVEF in both
groups of study.
40
(No Transcript)
41
(No Transcript)
42
- 14 pts with CAD(gt70 stenosis of at least one
coronary artery) and 12 normal subjects were
studied.
43
(No Transcript)
44
(No Transcript)
45
(No Transcript)
46
(No Transcript)
47
- In normal subjects, CSBF was 228 80 ml/min,
which increased to 540 246 ml/min (CFR 2.45
0.96). - In subjects with CAD the rest CSBF of 267 96
ml/min rose to 374 145 ml/min with DP (CFR1.50
0.41). The CFR was significantly lower in pts
with CAD (P 0.003).
48
- Our angiographic simultaneous study revealed that
echocardiographic assessment of CFR with Doppler
was comparable to findings elucidated by
angiography.
49
- We conclude that CSBF may be measured using TTE.
- We also conclude CFR measurements
- made by TTE are significantly reduced
- in pts with CAD.
- Echocardiographic assessment of CFR with Doppler
was comparable to findings elucidated by
angiography. - These findings suggest that TTE may be used as a
noninvasive method to diagnose CAD.
50
- Echocardiography. Nov14(6 Pt 1)579-588.
- Transesophageal Doppler Analysis of Coronary
Sinus Flow A New Method to Assess the Severity of
Tricuspid Regurgitation. - Zamorano J, AlmerÃa C, Alfonso F, Angeles Perez
M, Grauper C, Morales R, SÃnchez-Harguindey L. - Madrid, Spain
51
- BACKGROUND
- Severe MR induces reversal of flow in the PVs. We
hypothesized that severe TR may disrupt normal CS
flow. The purpose of this study was to analyze
the Doppler flow pattern of the CS and to
determine its value in the assessment of the
severity of TR.
52
- METHODS
- The CS flow was analyzed in 70 consecutive pts
with some degree of TR (27 mild, 14 moderate,
and 29 severe) and in 35 pts without TR. The CS
flow was obtained by TEE-PW .
53
- In pts without or with only mild TR the CS
Doppler flow pattern was formed by 2 negative
waves, a late systolic wave and another diastolic
wave.
54
The systolic wave became reversed in 21 (96) of
the pts with severe TR. The sensitivity,
specificity, and diagnostic accuracy of the
presence of a reversed systolic wave in the CS
for the diagnosis of severe TR was 95, 82, and
80, respectively.
55
CONCLUSIONS Significant TR modifies the CS
flow pattern as assessed by TEE. The presence of
a reversed systolic flow in the CS appears to be
a reliable new sign with good sensitivity,
specificity, and diagnostic accuracy for the
diagnosis of severe TR.
56
Original article Echocardiographic evaluation of
the coronary sinus MDItzhak Kronzon et
al. Department of Medicine, New York, USA
57
- The purpose of this study was to compare TTE and
TEE in the evaluation of the CS and its blood
flow.
58
- TEE is superior to TTE in the evaluation of the
coronary sinus and its blood flow velocity.
59
Thanks
Recommended
CrystalGraphics Presentations





























