
Antiemetics - PowerPoint PPT Presentation
1 / 25
Title:
Antiemetics
Description:
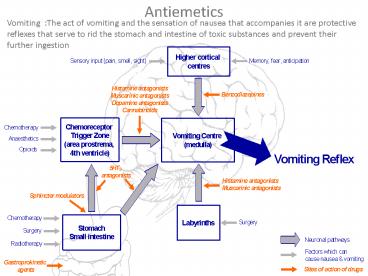
Vomiting :The act of vomiting and the sensation of nausea that accompanies it are protective reflexes that serve to rid the stomach and intestine of toxic substances ... – PowerPoint PPT presentation
Number of Views:563
Avg rating:3.0/5.0
Title: Antiemetics
1
Antiemetics
Vomiting The act of vomiting and the sensation
of nausea that accompanies it are protective
reflexes that serve to rid the stomach and
intestine of toxic substances and prevent their
further ingestion
2
Pathophysiology of Emesis
Cerebral cortex
Cancer chemotherapy Opioids
Smell Sight Thought
Anticipatory emesis
Chemoreceptor Trigger Zone (CTZ)
Vestibular nuclei
Vomiting Centre (medulla)
Motion sickness
Muscarinic Histaminic H1
Muscarinic, 5 HT3 Histaminic H1
(Outside BBB)
Dopamine D2 5 HT3,,Opioid Receptors
Chemo radio therapy Gastroenteritis (vagus)
Pharynx GIT
5 HT3 receptors
3
Area Type of receptors Stimulus
Chemoreceptor trigger zone (CTZ) Dopamine D2 5HT3 Opioid Cancer chemotherapy Opioids
Vestibular nuclei Mscarinic Histamine H1 Motion sickness
Pharynx and GIT 5HT3 Cancer chemotherapy Radio therapy Gastroenteritis
Cerebral cortex Smell Sight Thought Anticipatory emesis
Serotonin 5HT3 receptor antagonists 5HT3 receptor
Phenothiazines Dopamine D2 receptors Antihistaminic Anticholinergic
Substituted benzamides Dopamine D2 receptors
Anticholinergic drugs Muscarinic receptors
Antihistaminic drugs Histamine H1 receptors
4
Indications of antiemetics
- 1- Chemotherapy-induced vomiting
- 2- Post irradiation vomiting
- 3- Postoperative vomiting
- 4- Vomiting of pregnancy
- 5- Motion sickness
Group of drugs used as antiemetics
Serotonin 5 HT3 Antagonists Dopamine D2
Antagonist Anticholinergics H1 Antihistaminics
5
- Serotonin 5 HT3 Antagonist
- Potent antiemetics
Mechanism of action 1- Peripheral 5-HT3 receptor
blockade on intestinal vagal afferents. 2-
Central 5-HT3 receptor blockade in the vomiting
center and chemoreceptor trigger zone
Antiemetic action is mainly against Emesis
mediated by vagal stimulation (e.g. postoperative
and chemotherapy) High first pass
metabolism Excreted by liver kidney No dose
reduction in renal insufficiency but needed in
hepatic insufficiency
6
Drugs Available
- Ondansetron
- Granisetron
- Dolasetron
- Palonosteron
Adverse Effects
The most common adverse effects are 1- Headache
and dizziness 2- Constipation or diarrhoea
Indications
- Chemotherapy induced nausea and vomiting
- postradiation nausea vomiting
- Vomiting of pregnancy
- Postoperative vomiting
7
Corticosteroids
- Corticosteroids have antiemetic properties
- Mechanism of action possibly by suppressing
peritumoral inflammation and prostaglandin
production. - Use to enhance efficacy of 5HT3 receptor
antagonists in the treatment of
chemotherapy-induced vomiting.
8
Phenothiazines
- Phenothiazines as promethazine are antipsychotic
agents - Use
- Chemotherapy-induced vomiting
- Radiotherapy-induced vomiting
- postoperative nausea and vomiting
- Mechanism of the antiemetic action inhibition of
central dopamine, muscarinic and H1 histamine
receptors receptors
9
Butyrophenones
- Butyrophenones as droperidole are antipsychotic
agents - Mechanism of the antiemetic action inhibition of
central dopamine receptors - Use
- Chemotherapy-induced vomiting
- Radiotherapy-induced vomiting
- postoperative nausea and vomiting
- Adverse effects droperidol may prolong the QT
inter, therefore, it should not be used in
patients with QT prolongation (should only be
used in patients who have not responded
adequately to alternative agents).
10
Substituted Benzamides
- 1- Metoclopramide
- 2- Trimethobenzamide
- Mechanism of antiemetic action Central
dopamine-receptor blockade - Side effects (mainly extrapyramidal)
- Restlessness
- Dystonias
- Parkinsonian symptoms
11
H1 receptor antagonists and Anticholinergics
- Use
- prevention or treatment of motion sickness.
- Adverse effects sedation, dizziness,confusion,
dry mouth, cycloplegia, and urinary retention. - .
Diphenhydramine dimenhydrinate First generation H1 receptor blockers that have anticholinergic and sedating properties
Meclizine First generation H1 receptor blockers that have lesser anticholinergic and sedating properties
Hyoscine Muscarinic receptor blocker
12
Benzodiazepines
- Uses
- Benzodiazepines such as diazepam are used prior
to the initiation of chemotherapy to reduce
anticipatory vomiting or vomiting caused by
anxiety
13
Cannabinoids(Dronabinol)
- The mechanisms for the antiemetic effects is not
known. - Pharmacokinetics.
- readily absorbed after oral administration
- It undergoes extensive first-pass metabolism
with limited systemic bioavailability after
single doses Mmetabolites are excreted primarily
via the biliary-fecal route - Adverse effects include
- Euphoria or dysphoria, sedation and
hallucinations - Abrupt withdrawal leads o withdrawal syndrome
(restless, insomnia and irritability) - Autonomic effects (sympathetic) in the form of
tachycardia, palpitation, conjunctival injection,
and orthostatic hypotension. - Use
- For the prevention of chemotherapy-induced nausea
and vomiting
14
Control of GIT motility
- Neurogenic control of GIT moyility the ENS
- Enteric nervous system (ENS) is a collection of
nerves within the wall of the GI tract
responsible for the autonomous gastrointestinal
activity. It consists of connected networks of
neurons - myenteric (Auerbach's) plexus, found between the
circular and longitudinal muscle layers
(responsible for motor control) - submucosal (Meissner's) plexus, found below the
epithelium (regulates secretion, fluid
transport, and vascular flow). - Neurons in both plexuses release
acetylcholine at their terminals. - Autonomic nervous system
- Parasympathetic act by releasing
acetylcholine at nerve terminals. It causes
contraction of muscles in the wall of the
intestine and relaxation of the sphincters and
increases gland secretion - Sympathetic act by releasing
norepinephrine at nerve terminals. It causes
relaxation of muscles in the wall of the
intestine and contraction of the sphincters - Types of cholinergic receptors are M2 and M3
(present in the GIT in a 41 ratio). M3 receptor
is more important in muscle contraction.
15
Agents that increase GIT motility
- 1- Cholinergic agents
- Stimulate cholinergic receptors. Enhance
contractions in an uncoordinated manner that
produces no net propulsive activity. Not useful
for treating motility disorders - 2- Prokinetic agents
- enhance coordinated GIT propulsive motility.
Prokinetic agents act at receptor sites on the
motor neuron itself increasing the release of
acetylcholine at the motor nerve terminal without
interfering with the normal physiological pattern
and rhythm of motility. Useful for treating
motility disorders
16
Cholinergic Agents
- Direct cholinergic agents
- Stimulate cholinergic receptors in the wall of
the GIT. - 1- ACh is not used pharmacologically because
- it affects both nicotinic and muscarinic
receptors - It is degraded rapidly by acetylcholinesterase.
- 2- Bethanechol
- Muscarinic receptor agonist
- Resists enzymatic hydrolysis.
- In addition, it lacks real prokinetic
efficacy,
17
- Indirect cholinergic agents
- Acetylcholinesterase Inhibitors. These drugs
inhibit the degradation of ACh , allowing ACh to
accumulate at sites of release. - Neostigmine has been used to treat paralytic
ileus.
18
Decreased motility of GIT
- Decreased motility of the GIT results from
suppression of ACh release from myenteric motor
neurons mediated by stimulation of D2
dopaminergic receptors.
19
Prokinetic agents
- Enhance coordinated GI T propulsive motility.
- Mechanism of action
- 1- Antagonize the inhibitory effect of
dopamine on myenteric motor neurons, - 2- Relieve nausea and vomiting by
antagonism of dopamine receptors in the
chemoreceptor trigger zone - Metoclopramide
- Domperidone.
20
Substituted benzamides1- Metoclopramide (1)
- Pharmacological action
- 1- Enhance coordinated GIT propulsive motility of
the upper digestive tract where it increases
lower esophageal sphincter tone and stimulates
antral and small intestinal contractions.
Metoclopramide has no clinically significant
effects on motility of the colon. - Mechanisms of action (on GIT)
- dopamine receptor antagonism
- 5-HT4-receptor agonist
- vagal and central 5-HT3-antagonist
- sensitization of muscarinic receptors on smooth
muscle - 2- Antiemetic action
- Mechanism of action
- Antagonize dopamine receptors in the CTZ
21
1- Metoclopramide (2)
- Therapeutic Use
- Nausea and vomiting that often accompany GI
dysmotility syndromes. - Gastroesophageal reflux disease (symptomatic
relief but not healing of esophagitis). - Gastroparesis where it improves gastric
emptying. - Diagnostic procedures such as intestinal
intubation or contrast radiography of the GI
tract. - Postoperative ileus
- Persistent hiccups
22
1- Metoclopramide (3)
- Administration
- 1- Oral (rapid absorption)
- 2- I.m. in cases of nausea and vomiting
- 3- I.v. infusion in chemotherapy-induced vomiting
23
1- Metoclopramide (4)
- Adverse Effects
- 1- Extrapyramidal effects (more commonly in
children and young adults and at higher doses). - Tardive dyskinesiarepetitive,
involuntary, purposeless movements (usually
involve the face) like tongue protrusion, lip
smacking, pursing of the lips and rapid eye
blinking. It occurs with chronic treatment
(months to years) and may be irreversible - Akathisia restlessness and inability to
sit still or remain motionless - Dystonias muscular spasms of neck
usually occurring acutely after intravenous
administration - parkinsonian-like symptoms that may occur
several weeks after initiation of therapy
generally respond to treatment with
anticholinergic or antihistaminic drugs and are
reversible upon discontinuation of
metoclopramide. - 2- Galactorrhea by blocking the inhibitory
effect of dopamine on prolactin release
(infrequent)
24
2- Domperidone
- Pharmacological actions
- 1- Enhance coordinated GIT propulsive motility of
the upper digestive tract where it increases
lower esophageal sphincter tone and stimulates
antral and small intestinal contractions. It
has no clinically significant effects on motility
of the colon. - Mechanism of action
- dopamine D2 receptor antagonist
- 2- Antiemetic action
- Mechanism of action
- dopamine D2 receptor antagonist (of D2 receptors
in CTZ which is outside BBB)
25
- Adverse effects
- No extrapyramidal side effects (can not cross the
blood-brain barrier) - Galactorrhea (by inhibiting dopamine-mediated
inhibition of the release of prolactin as the
pituitary lacks blood-brain barrier)