
Hip Joint - PowerPoint PPT Presentation
1 / 30
Title:
Hip Joint
Description:
Medial & lateral circumflex arteries usually arise from the profunda femoris; ... The medial circumflex is usually the major supply; it passes beneath the ... – PowerPoint PPT presentation
Number of Views:237
Avg rating:3.0/5.0
Title: Hip Joint
1
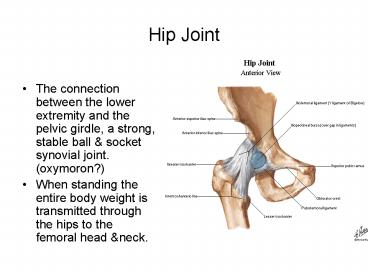
Hip Joint
- The connection between the lower extremity and
the pelvic girdle, a strong, stable ball socket
synovial joint. (oxymoron?) - When standing the entire body weight is
transmitted through the hips to the femoral head
neck.
2
Articular surfaces
- Femoral head- approximately 2/3rds of a sphere
except for the pit of the fovea. The head is
covered by articular cartilage, thicker over the
weight nearing areas. - Fovea
- Ligament of the head
3
- Acetabulum the hollow cup for the femoral head
located on the lateral aspect of the hip. - Acetabular rim fibrocatrilagenous lip with an
inferior defect in the rim segment (acetabular
notch). - Lunate surface of the acetabulum is the weight
bearing surface covered by articular cartilage, - Acetabular labrum a lip of fibrocatilage that
increases the depth of the acetabulum, it allows
the acetabulum to grip the femoral head beyond
the equator. - Transverse acetabular ligament bridges the
acetabular notch
4
- Acetabular fossa the non-articular part of the
acetabulum formed by the ischium - The articular surface of the acetabulum femoral
head are most congruent when the hip is flexed at
90, abducted 5 and laterally rotated 10. This
is the quadruped position.
5
(No Transcript)
6
Joint capsule
- Formed by a strong loose external fibrous layer
and an internal synovial membrane. - External fibrous layer
- Attaches proximally on the hip bone to the rim of
the acetabulum transverse acetabular ligament. - Distally attaches to the femoral neck only
anteriorly at the intertrochanteric line the
root of the greater trochanter, posteriorly the
fibrous layer has an arched border that crosses
the neck proximal to the intertrochanteric crest
it is not attached to the neck. - Posteriorly the synovial membrane extends beyond
the free posterior margin of the joint capsule on
the femoral neck, it forms a bursa for the
obturator externus.
7
(No Transcript)
8
- 4. Fibers of the fibrous layer take a spiral
course from the hip bone to the intertrochanteric
line. - 5. Orbicular zone deep fibers present on the
posterior capsule wind circularly around the
femoral neck. - 6. Thickened parts of the fibrous layer form
ligaments which pass a spiral fashion from the
pelvis to the femur. - 7. Extension tightens the spiral ligaments
fibers, constricts the capsule pulls the
femoral head into the acetabulum. This limits
extension to 10-20 beyond vertical. Flexion
unwinds the ligaments allows increasing hip
mobility
9
(No Transcript)
10
Hip Joint Reinforcement
- Anteriorly superiorly Strengthened by a
Y-shaped iliofemoral ligament, attaches from the
AIIS rim anteriorly and intertrochanteric line
distally, this is the strongest ligament in the
body. The iliofemoral ligament specifically
prevents hyperextension of the hip while
standing. - Anteriorly inferiorly The pubofemoral ligament
arises from the obturator crest of the pubic bone
passes laterally inferiorly to merge with the
fibrous layer of the joint capsule. The ligament
blends with the medial part of the iliofemoral
ligament. It tightens during extension
abduction of the hip, it prevents over abduction
of the hip joint. - Posteriorly The weak ischiofemoral ligament
arises from the ischial part of the acetabular
rim spirals superiolaterly to the neck of the
femur, medial to the base of the greater
trochanter.
11
(No Transcript)
12
(No Transcript)
13
- Figure 5-52B depicts the location and strength of
hip muscles and ligaments. The muscles and
ligaments pull the femoral head medially into the
acetabulum. - Medial lateral rotators of the thigh function
to pull the femoral head into the acetabulum. - Medial flexors (located anteriorly) are weaker
and have poor mechanical advantage but associated
ligaments are stronger. - Medial extensors (located posteriorly) are
stronger with more mechanical advantage but
associated ligaments are weaker.
14
Synovial membrane of the Hip Joint
- The synovial membrane lines the fibrous joint
capsule intercapsular bony surfaces not lined
by articular cartilage. - The membrane reflects proximally along the
femoral neck - Synovial folds (retincaula) reflect superiorly
along the femoral neck as longitudinal bands.
These contain subsynovial retinacular arteries
(consist of medial and a few lateral circumflex
artery branches) that supply the femoral head
neck
15
- Ligament of the head of the Femur A synovial
fold conducting a vessel to the head of the
femur, this forms a weak ligament. The artery is
important developmentally but is unable to
adequately supply the mature femoral head. The
wide end attaches to the acetabular margins the
transverse acetabular ligament. The narrow end
attaches to the fovea for the ligament of the
femoral head. - A fat pad fills in the acetabular fossa not
filled by the ligament of the head, the pad
changes shape to accommodate head movements. The
fat pad ligament of the head are covered by a
synovial membrane.
16
- The synovial membrane protrudes beyond the free
margin of the joint capsule on the posterior
aspect of the femoral neck forms a bursa for
the obturator externus muscle
17
Hip Movements
- Flexion/extension at the hip depends on knee
position, knee flexion releases the hamstring and
thigh flexion increases until it reaches the
anterior abdominal wall. - Extension The fibrous capsule of the joint
especially the iliofemoral ligament is taut. Hip
extension is limited by the iliofemoral ligament. - Abduction is freer than adduction. It can reach
60 with the thigh extended and increases when
the thigh is flexed. - Lateral rotation is more powerful than medial
rotation
18
(No Transcript)
19
Hip Movements
- Strongest flexor is the iliopsoas muscle
- Adduction flexion by the adductor magnus
(adductor portion) brevis and longus, pectineus
and gracillis - Adduction extension by the hamstring part of
the adductor magnus - Abduction media rotation anterior portion of
the gluteus medius minimus - Primary extensor of the hip is the gluteus
maximus particularly when extending the thigh
from a flexed position, after the leg is straight
the hamstrings become the primary extensors.
20
Blood Supply to the Femoral head Neck
- Medial lateral circumflex arteries usually
arise from the profunda femoris they may arise
from the femoral artery - The medial circumflex is usually the major
supply it passes beneath the unattached
posterior border of the joint capsule to supply
the head neck via retinacular arteries. - The artery to the femoral head is a branch of the
obturator artery and travels to the head in the
ligament of the head this is important
developmentally but is inadequate to supply the
mature head neck.
21
(No Transcript)
22
Nerve Supply follows Hiltons Law
- Flexors are innervated by the femoral nerve and
pass anteriorly to the hip joint and supply the
anterior aspect of the hip joint. - Lateral rotators pass inferiorly posteriorly to
the joint, the obturator sends branches the
inferior aspect and the nerve to the quadratus
femoris supplies the posterior aspect of the
joint. - Adductors supplied by the superior gluteal nerve
(glut. Medius minimis) pass superiorly to the
joint so this area is supplied by the superior
gluteal nerve
23
Hip dislocations
- Dislocation of the femoral head is unusual due to
the stability of the joint, this requires a
significant force. - This occurs most often when the hip is flexed and
medially rotated the usual position of the lower
limb when riding in an automobile. The dashboard
compresses the knee which causes the femoral head
to rupture through the weaker posterior margin of
the joint capsule. - Posterior dislocations are much more common than
anterior dislocations. Given its proximity
sciatic nerve injury is often associated with
posterior dislocations. - Anterior dislocation of the hip requires the
application of force the hip in extension,
abduction and lateral rotation (when catching a
tip in snow skiing. Often these injuries are
accompanied by fractures of the acetabular
margins and disruption of the acetabular labrum.
24
- The posteriorly dislocated hip is slightly flexed
at the thigh knee with medial rotation.
25
(No Transcript)
26
- Posterior hip dislocations are frequently
accompanied by fractures of the acetabulum.
27
- Although a true hip fracture involves the joint,
the following four proximal femur fractures are
commonly referred to as 'hip fractures'. The
differences between them are important because
each is treated differently. - Femoral head fracture denotes a fracture
involving the femoral head. This is usually the
result of high energy trauma and a dislocation of
the hip joint often accompanies this fracture. - Femoral neck fracture (sometimes Neck of Femur
(NOF), subcapital, or intracapsular fracture)
denotes a fracture adjacent to the femoral head
in the neck between the head and the greater
trochanter. These fractures have a propensity to
damage the blood supply to the femoral head,
potentially causing avascular necrosis. - Intertrochanteric fracture denotes a break in
which the fracture line is between the greater
and lesser trochanter on the intertrochanteric
line. It is the most common type of 'hip
fracture' and prognosis for bony healing is
generally good if the patient is otherwise
healthy. - Subtrochanteric fracture actually involves the
shaft of the femur immediately below the lesser
trochanter and may extend down the shaft of the
femur
28
(No Transcript)
29
Acetabular Fractures
30
hip replacement
Recommended
CrystalGraphics Presentations





























