
Maxillofacial Trauma Dentoalveolar fractures - PowerPoint PPT Presentation
1 / 16
Title:
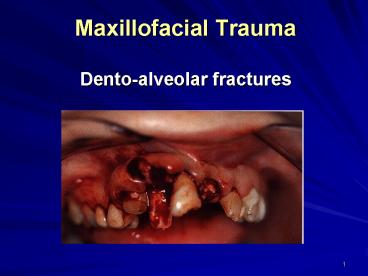
Maxillofacial Trauma Dentoalveolar fractures
Description:
... 3 times at risk than girls (Hunter et al 1990, Andreason ... Finger manipulation. Reduction (closed ) and fixation. Rigid wire and composite splint ... – PowerPoint PPT presentation
Number of Views:2726
Avg rating:3.0/5.0
Title: Maxillofacial Trauma Dentoalveolar fractures
1
Maxillofacial TraumaDento-alveolar fractures
2
Definition
- Are those in which avulsion, subluxation or
fracture of the teeth occurs in association with
a fracture of the alveolus - It may occur as an isolated clinical entity or in
conjunction with any other soft tissue or facial
bone fracture - Isolated dento-alveolar fracture seen among
children and adolescents and boys are 3 times at
risk than girls (Hunter et al 1990, Andreason
Andreason 1994)
3
Etiology
- RTA (minor accidents)
- Collisions and falls
- Cycling accidents
- Epileptic seizures
- Iatrogenic damage during
- Extraction of teeth
- Endoscopy procedure
- Endotreacheal intubation
4
Classification of dento-alveolar
injuries(Andreasen Andreasen 1994)
- Dental hard tissue injury
- Crown infracture and fracture with or without
root fracture - Periodontal injury
- Concussion, subluxation, intrusion, extrusion,
lateral luxation, avulsion - Alveolar bone injury
- Intrusion of teeth with fracture of socket,
alveolus or jaws - Gingival injury
- contusion, abrasion, laceration, degloving
- Combination of the above
5
Dental hard tissue injury
- Occurs as a result of direct trauma or by
forcible impaction against the opposing dentition - Anterior teeth damaged by direct impact while
posterior ones damaged by impaction between the
two jaws - Upper teeth intrusion are more frequent and
impact against lower teeth may lead to vertical
splitting - Meticulous clinical and radiographical
examination are very essential to determine the
degree of dental damage and chest x-ray when
missing or knocked out tooth is suspected - Early treatment is imperative to relieve pain and
preserve tooth
6
Treatment objectives
- Preservation of damaged teeth depends on
- Complexity of maxillofacial injury
- Age of the patient
- General dental condition
- Site of injury
- Wishes of the patient
- Prognosis is influenced by
- Open root apices
- Intact gingival tissue
- Absence of root fracture
- periodontal-bone support
7
Injuries to the primary dentition
- 70 involve maxillary central incisors
- Intrusion, lateral luxation and avulsion are the
commonest - Intruded teeth are likely to normally erupt
spontaneously - Damage to developing permanent teeth by displaced
tooth are recognizable problem - Management
- Fractured, extruded or grossly displaced teeth
are to be extracted - Less displaced with no occlusal interference
should be monitored since extraction carries risk
to permanent one
8
Management of injuries to permanent dentition
- Crown fracture
- Dressing of exposed dentin, minimal pulpotomy
or pulp extirpation and restoration of damaged
part of the tooth - Root fracture
- (Oblique, vertical or
transverse) - Inevitable extraction
- Saving the tooth by
- Rigid splinting for a minimum of 8 weeks
- Devitlaiztion (RCT) with eventful apico surgery
- Orthodontic extrusion or crown lengthening
9
Injuries to periodontal tissues
- Force distributed over several teeth or impact
cushioned by overlying soft tissue may result
into - Concussion
- Subluxation
- Intrusion
- Displacement and avulsion
- Fracture of teeth structure
- Looseness and displacement of teeth carries a
high risk of subsequent pulp necrosis - As with root fracture, late complications can be
resorption, canal obliteration, ankylosis and
loss of alveolar bone
10
Management of injuries to the periodontal tissues
- Loosened, laterally luxated and extruded teeth
should be repositioned and splinted for 1-3 weeks
respectively by semi rigid splint - Acid-etch composite
- Arch bar
- Orthodontic wire
- Soft stainless-steel wire-loop,
- Vacum formed splint
- Avulsed teeth necessities immediate replantation
and semi-rigid splinting for 1-2 weeks and
prognosis is influenced by - stage of root development
- length of exposure
- medium storage
- handling and splinting
11
Alveolar fracture
- Alveolar injury in mandible is associated with
complete fracture of tooth-bearing area and in
maxilla is often isolated injury - Teeth damage might be no existed but the
potential devitilzation should be expected - Alveolar fractures are often seen as two distinct
fragment containing teeth but comminuted fracture
is possible - Alveolar fracture in mandible my go along with
mandible fracture and impacted fracture into the
maxilla may appear to be immobile - Midline split of palate with unilateral Le Fort I
lead to large dento-alveolar fracture - Fracture of tuberosity and fracture of antral
floor is a recognized complication of upper
molars extraction
12
Management of injuries to the alveolar
bone(Block or plate fracture)
- Finger manipulation
- Reduction (closed ) and fixation
- Rigid wire and composite splint
- Elimination of premature contact and occlusal
trauma - Short inter-maxillary fixation
13
Management of tuberosity fracture
- Removal of comminuted fracture of loss alveolar
bone and teeth and repair of soft tissue - Delay of extraction of teeth in case of
tuberosity fracture for (6-8 weeks) - Mandatory extraction of a tooth from a block
fracture should be carried out surgically - Splinting of a tooth of fractured tuberodity in
to other standing teeth for one month
14
Injuries to the gingival and soft tissues
- Damage to the lip observed more with anterior
dento-alveolar fracture - Embedded of portion of a tooth or foreign bodies
in soft tissues is very substantial - Laceration of the gingiva is associated with
dento-alveolar fracture - Degloving of the mental region is a common injury
to the lower anterior teeth
15
Management of soft tissue injuries
- Inspection of a full thickness perforating wound
- Debridment and copious lavage
- with cholohexidine solution
- Removal of denuded piece of bone
- Repair of soft tissue injury
- Application of external support strapping to help
in tissue adaptation - Antibiotic prescription
16
(No Transcript)
Recommended
CrystalGraphics Presentations





























