
Endocarditis caused by Cardiobacterium valvarum in a Patient with - PowerPoint PPT Presentation
1 / 1
Title:
Endocarditis caused by Cardiobacterium valvarum in a Patient with
Description:
2. Han XY, Meltzer MC, Woods JT, and Fainstein V. 'Endocarditis with Ruptured ... The chest pain, which began the morning of admission, was described as severe ... – PowerPoint PPT presentation
Number of Views:177
Avg rating:3.0/5.0
Title: Endocarditis caused by Cardiobacterium valvarum in a Patient with
1
Endocarditis caused by Cardiobacterium valvarum
in a Patient with Bicuspid Aortic Valve and
Severe Aortic Insufficiency
Garrett M. Chinn Richard R. Jahan-Tigh David S.
Yoho, MD1 Joseph Timpone, MD2
1Department of Medicine, Inova Fairfax Hospital,
Fairfax, VA 2Department of Medicine, Georgetown
University Hospital, Washington, DC
Georgetown University
Abstract
Imaging
The Cardiobacterium genus is a rare cause of
infectious endocarditis. The recent
characterization of Cardiobacterium valvarum has
been accompanied by case reports of endocarditis
caused by this organism. We report a case of
HACEK endocarditis caused by Cardiobacterium
valvarum in an individual with bicuspid aortic
valve and ascending aortic dilatation who
presented with acute myocardial infarction.
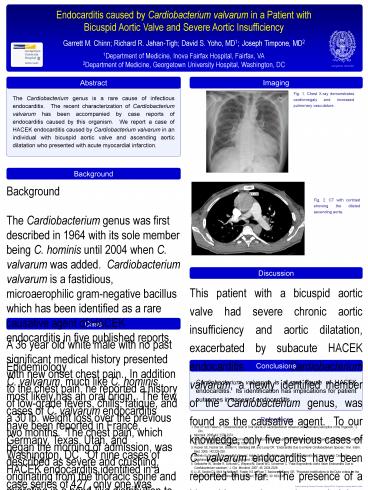
Fig. 1. Chest X-ray demonstrates cardiomegaly and
increased pulmonary vasculature.
Background
Background The Cardiobacterium genus was first
described in 1964 with its sole member being C.
hominis until 2004 when C. valvarum was added.
Cardiobacterium valvarum is a fastidious,
microaerophilic gram-negative bacillus which has
been identified as a rare causative agent of
HACEK endocarditis in five published
reports. Epidemiology C. valvarum, much like C.
hominis, most likely has an oral origin. The few
cases of C. valvarum endocarditis have been
reported in France, Germany, Texas, Utah, and
Washington, DC. Of nine cases of HACEK
endocarditis identified in a case series of 427,
only one was identified as C. hominis,
demonstrating the rarity of Cardiobacterium as a
cause of endocarditis. Pathogenesis The majority
of reported cases of C. valvarum endocarditis
involved bicuspid aortic valves, severe valvular
destruction with associated vegetations, and
resultant aortic insufficiency with stigmata of
infectious endocarditis. A history of a recent
dental procedure was implicated in most cases as
the inciting event. Diagnosis Culture on
sheeps blood agar in a microaerophilic
environment reveals an organism which has
variable hemolytic activity and is cytochrome
oxidase and H2S-producing positive. It is
negative for catalase, urea hydrolysis, esculin
hydrolysis, and nitrite reduction. Indole
production varies by strain. API 20NE and NH
assays may result in misidentification. Cellular
fatty analysis and 16s rRNA gene sequencing can
differentiate C. valvarum from C. hominis.
Fig. 2. CT with contrast showing the dilated
ascending aorta.
Discussion
This patient with a bicuspid aortic valve had
severe chronic aortic insufficiency and aortic
dilatation, exacerbated by subacute HACEK
endocarditis. Cardiobacterium valvarum, a newly
identified member of the Cardiobacterium genus,
was found as the causative agent. To our
knowledge, only five previous cases of C.
valvarum endocarditis have been reported thus
far. The presence of a bicuspid aortic valve,
indolent progression of symptoms, destructive
valvular vegetations, and aortic insufficiency
are consistent with these reports. While our
patient did not have a history of any recent
dental procedure, his poor dentition suggests his
oral flora as a possible source of his infection.
This case supports a growing body of evidence
that places C. valvarum as an extremely rare
cause of endocarditis which should be
increasingly recognized as molecular techniques
for species differentiation become more readily
available. As such, species differentiation may
allow us to identify patient populations
especially susceptible to C. valvarum
endocarditis, characterize differences in
pathology and presentation, and positively affect
patient outcomes.
Case
A 36 year old white male with no past significant
medical history presented with new onset chest
pain. In addition to the chest pain, he reported
a history of low-grade fevers, chills, fatigue,
and a 30 lb. weight loss over the previous two
months. The chest pain, which began the morning
of admission, was described as severe and
crushing, originating from the thoracic spine and
migrating in a band-like distribution to the
anterior left chest wall and left arm. The
patients primary care physician had previously
told him he had an enlarged heart and anemia, for
which he was started on iron supplementation.
There was no history of recent dental work and he
vaguely recalled having a cardiac murmur present
since childhood. On admission, temperature was
98.7 and blood pressure was 106/51. Physical
exam revealed a pale, cachectic appearing male
with poor dentition. Cardiac exam was
significant for grade II/VI systolic and
diastolic murmurs at the left sternal border. Of
note, Quinckes pulses, Duroziezs sign, and de
Mussets sign were present. Pulmonary exam was
without wheezes, rales, or rhonchi. Digital
clubbing was present. Hemoglobin was 9.7g/dL,
white blood count was 7,400/µL, and troponins
were positive. EKG showed a 1st degree A-V block
and a chest X-ray revealed cardiomegaly. Chest
CT with contrast showed an aortic root dilatation
measuring 5.1 cm and ascending aorta dilatation
measuring 6.1 cm. Transthoracic and
transesophageal echocardiographies demonstrated
marked left ventricular enlargement with ejection
fraction of 50-55 without diastolic dysfunction
and no dissection noted in the dilated aorta.
Echocardiography also showed a probable
non-stenotic bicuspid aortic valve with severe
insufficiency via a main regurgitant jet and a
perforating jet through a fused left-posterior
cusp. No vegetations were seen on either aortic
or mitral valves. When stable, the patient was
taken to the operating room for bioprosthetic
aortic valve replacement and Hemashield graft of
the ascending aorta. Aortic and mitral annular
abscesses were found and debrided. Two sets of
blood cultures drawn six hours apart on the day
of admission grew gram-negative bacilli after 45
hours, later identified as Cardiobacterium
valvarum by the Commonwealth of Virginia Division
of Consolidated Laboratory Services. The patient
recovered well post-procedure and was discharged
on ceftriaxone 2g IV daily for six weeks.
Conclusions
Cardiobacterium valvarum is a rare cause of
HACEK endocarditis. Its identification has
implications for patient outcomes in cases of
endocarditis.
References
1. Han XY and Falsen E. Characterization of Oral
Strains of Cardiobacterium valvarum and Emended
Description of the Organism, J. Clin.
Microbiol. 2005 43 2370-2374. 2. Han XY,
Meltzer MC, Woods JT, and Fainstein V.
Endocarditis with Ruptured Cerebral Aneurysm
Caused by Cardiobacterium valvarum sp. nov.,
J. Clin. Microbiol. 2004 42 1590-1595. 3.
Hoover SE, Fischer SH, Shaffer R, Steinberg BM,
and Lucey DR. Endocarditis Due to a Novel
Cardiobacterium Species, Ann. Intern. Med.
2005 142229-230. 4. Bothelo E, Gouriet F,
Fournier P-E, Roux V, Habib G, Thuny F, Metras D,
Raoult D, and Casalta J-P. Endocarditis Caused
by Cardiobacterium valvarum, J. Clin.
Microbiol. 2006 44 657-658. 5. Geibdorfer W,
Tandler R, Schlundt C, Weyand M, Daniel WG,
Schoerner C. Fatal Bioprosthetic Aortic Valve
Endocarditis Due to Cardiobacterium
valvarum, J. Clin. Microbiol. 2007 45
2324-2326. 6. Li JS, Sexton DJ, Mick N, Nettles
R, Fowler VG Jr, Ryan T, Bashore T, Corey GR.
Proposed modifications to the Duke criteria for
the diagnosis of infectious endocarditis,
Clin. Infect. Dis. 2000 30 633-638.