
Pituitary Apoplexy - PowerPoint PPT Presentation
1 / 16
Title: Pituitary Apoplexy
1
(No Transcript)
2
(No Transcript)
3
(No Transcript)
4
(No Transcript)
5
(No Transcript)
6
(No Transcript)
7
Pituitary Apoplexy
- Kyla Lokitz
- Morning Report
- 7/18/05
8
Pituitary Apoplexy
- A clinical syndrome resulting from acute
hemorrhage or infarction of the pituitary gland
characterized by the onset of - Headache
- Vomiting
- Visual Disturbances
- Opthalmoplegia CN III most common
- Meningismus
- Fever
- Decreased Consciousness
- Death
9
Epidemiology
- Incidence found to be 0.6-9.0 in series of
surgically treated adenomas in patients with
pituitary apoplexy (Semple et al. 2005). - Pituitary hemorrhage observed in 25 of
surgically removed adenomas however, these
patients were without clinical symptoms
(Subclinical Pituitary Apoplexy) (Sibal et al.
2005). - Hemorrhage and infarction with similar clinical
presentation described in nontumerous pituitary
glands. Also seen in other pituitary tumors such
as craniopharyngiomas and lymphocytic
hypophysitis. - Cases reported in patients in first through ninth
decade although pediatric cases rare. - Series suggest apoplexy occurs more frequently in
males (Lubina et al. 2005).
10
Predisposing Factors
- Arterial hypertension
- Sudden head trauma
- Cardiac surgery
- Transient elevation of intracranial pressure
- Diabetes
- Acromegaly
- Cushings Syndrome
- Estrogens
- Anticoagulation
- Bromocriptine
- Dynamic pituitary function tests
- GnRH analogues
- Radiotherapy
11
Pathophysiology
- With rapid growth, tumor outgrows blood supply
- Compression of the infundibular and superior
hypophyseal vessels against the diaphragma sellae - Ischemia of the normal pituitary gland
- Intrinsic vasculopathy of pituitary tumors
12
Diagnosis
- Laboratory Data
- Prolactin, TSH, FT4, FT3, Cortisol, LH, FSH,
Testosterone, Estrogen, GH, IGF1 - Electrolytes, CBC (patients often present with
hyponatremia and leukocytosis) - CSF-rbcs, xanthachromia, pleocytosis, increased
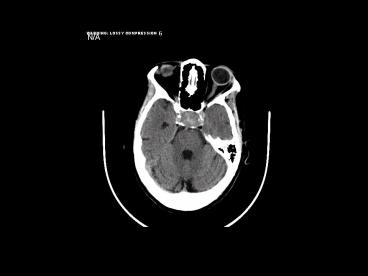
protein - Imaging
- X-ray may demonstrate enlarged sella
- CT will demonstrate pituitary mass but not
sensitive in demonstrating hemorrhage or
infarction (i.e. CT diagnostic in only 28 of
cases, defined sellar mass in 72 of cases)
(Sibal et al. 04) - MRI is the radiologic mode of choice (i.e.
confirmed diagnosis in gt90 of cases) (Sibal et
al. 04)
13
Treatment
- Careful monitoring of fluid and electrolyte
balance - Replacement of deficient hormone, especially
corticosteriods - Pituitary surgery
- Long term monitoring for hypopituitarism and
recurrence of pituitary adenomas
14
Surgical Treatment Indicated with
- Diminished level of consciousness
- Hypothalmic disturbances
- Visual impairment
- Some disagreement in literature about timing of
surgery question of improved outcome (in visual
field and visual acuity) if operation occurs
within 8 days of onset of symptoms (Randeva et
al. 1999) other studies demonstrate satisfactory
recovery of vision with late surgery (Ayuck et
al. 2004, Sibal et al. 2005).
15
Conservative Therapy
- Favored in patients without or with mild
neuro-opthalmic signs. - Retrospective studies have shown spontaneous
improvement in neuro-opthalmic symptoms with
conservative management (Sibal et al. 2005)
16
References
- Ayuck, J. et al. Acute management of pituitary
apoplexy surgery or conservative management?
Clinical Endocrinology 2004, 61 747-752. - Levy, A. et al. Pituitary Disease Presentation,
Diagnosis, and Management. J Neurol Neurosur
Psychiatry 2004, 751147-1152. - Lubina A. et al. Management of pituitary
apoplexy clinical experience with 40 patients.
Acta Neurochirugica 2005, 147151-157. - Ma, R. et al. Fever, headache, and a stiff neck.
The Lancet 2004, 363 1868. - Randeva, H. et al. Classical pituitary apoplexy
clinical features, management, and outcome.
Clinical Endocrinology 1999, 51181-188. - Semple, P. et al. Pituitary apoplexy.
Neurosurgery 2005, 56 65-73.
Recommended
CrystalGraphics Presentations





























