
Ischemic Heart Disease Chapter 17 - PowerPoint PPT Presentation
Title:
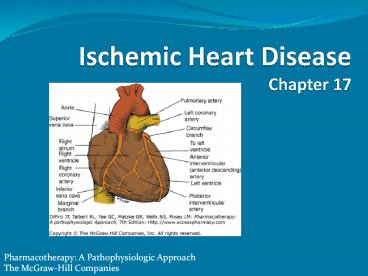
Ischemic Heart Disease Chapter 17
Description:
Pharmacotherapy: A Pathophysiologic Approach The McGraw-Hill Companies Table Footnotes aRefers to all patients diagnosed with CAD bMedical reasons for not prescribing ... – PowerPoint PPT presentation
Number of Views:2189
Avg rating:3.0/5.0
Title: Ischemic Heart Disease Chapter 17
1
Ischemic Heart DiseaseChapter 17
Pharmacotherapy A Pathophysiologic Approach
The McGraw-Hill Companies
2
Abbreviations
- ACC American College of Cardiology
- ACEI angiotensin-converting enzyme inhibitor
- ACIP Asymptomatic Cardiac Ischemia Pilot
- AHA American Heart Association
- AV arteriovenous
- CABG coronary artery bypass grafting
- CAD coronary artery disease
- CASS Coronary Artery Surgery Study
- CHD coronary heart disease
- CT computed tomography
- CVD cardiovascular disease
3
Abbreviations
- DCA directional coronary atherectomy
- ECG electrocardiogram
- EDRF endothelium-derived relaxing factor
- ETT exercise tolerance (stress) testing
- GMP guanosine monophosphate
- HDL high-density lipoprotein
- HERS Heart Estrogen/Progestin Replacement Study
- IHD ischemic heart disease
- I Na late sodium current
- ISDN isosorbide dinitrate
- ISMN isosorbide mononitrate
4
Abbreviations
- LAD left anterior descending
- LDL low-density lipoprotein
- LV left ventricle
- MI myocardial infarction
- MVO2 myocardial oxygen demand
- PCI primary coronary intervention
- PTCA percutaneous transluminal angioplasty
- R1 resistance 1-large epicardial or surface
vessels - R2 resistance 2-intramyocardial arteries and
arterioles
5
Key Concepts
- Ischemic heart disease (IHD) caused by coronary
atherosclerotic plaque formation which leads to
imbalance between O2 supply demand - results in myocardial ischemia
- Chest pain cardinal symptom of myocardial
ischemia caused by coronary artery disease (CAD) - Risk factor identification/modification important
interventions for patients with known/suspected
IHD
6
Key Concepts
- Major risk factors that can be altered
- dyslipidemia
- high total low-density lipoprotein cholesterol
- low high-density lipoprotein cholesterol
- high triglycerides
- smoking
- glycemic control in DM
- HTN
- therapeutic lifestyle changes
- exercise, weight reduction, reduced dietary
cholesterol - reduction in inflammation may play an important
role
7
Key Concepts
- Most CAD patients should receive antiplatelet
therapy - Manage chronic stable angina patients initially
with ß-blockers for symptomatic control - at least as well as nitrates or CCBs
- decrease risk of recurrent MI, CAD mortality
- Nitroglycerin, other nitrate products useful for
angina prophylaxis when patients undertake
activities known to provoke angina - When angina occurs on a regular, routine basis
- institute chronic prophylactic therapy
8
Key Concepts
- CCBs effective monotherapy
- generally used with ß-blockers or as monotherapy
for patients intolerant to ß-blockers - most patients with moderate to severe angina
require 2 drugs to control symptoms - ranolazine 2nd line drug
- used with ß-blockers CCBs
9
Key Concepts
- Pharmacologic management as effective as
revascularization if 1 or 2 vessels involved - no differences in survival
- recurrent MI
- other measures of effectiveness
- Multivessel involvement best managed with
revascularization - left main coronary artery disease
- left main equivalent disease
- 2- to 4-vessel involvement with significant left
ventricular dysfunction
10
Key Concepts
- Revascularization
- percutaneous transluminal coronary angioplasty
- coronary artery bypass graft (CABG)
- certain patients (e.g. diabetics) should have
CABG - Percutaneous transluminal coronary angioplasty
CABG produce similar results
11
Key Concepts
- Clinical performance measures for chronic stable
CAD - American College of Cardiology, American Heart
Association
- BP
- lipid profile
- drug therapy hyperlipidemia
- symptom activity assessment
- smoking cessation
- antiplatelet therapy
- ß-blocker therapy for prior myocardial infarction
- ACE inhibitor therapy
- diabetes screening
12
Ischemic Heart Disease
- Caused by epicardial vessel atherosclerosis which
leads to coronary heart disease - Presentation
- acute coronary syndrome
- chronic stable exertional angina pectoris
- ischemia without clinical symptoms
- heart failure, arrhythmias
- cerebrovascular disease
- peripheral vascular disease
13
Epidemiology
- 79 million American adults gt 1 type of
cardiovascular disease (CVD) - 2,400 Americans die of CVD each day
- average of 1 death every 33 seconds
- In 2004, CHD was responsible for 52 of CVD
deaths - Common initial presentation
- women angina
- men myocardial infarction
Rosamond W, Flegal K, Friday G, et al. Heart
disease and stroke statistics2007 update A
report from the American Heart Association
Statistics Committee and Stroke Statistics
Subcommittee. Circulation 200711569171.
14
Criteria for Determination of the Specific
Activity Scale Functional Class
Any Yes No
1. Can you walk down a flight of steps without stopping (4.5 5.2 MET)? Go to 2 Go to 4
2. Can you carry anything up a flight of 8 steps without stopping (5 5.5 MET)? Or can you a. Have sexual intercourse without stopping (5 5.2 MET) b. Garden, rake, weed (5.6 MET) c. Roller skate, dance foxtrot (5 6 MET) d. Walk at a 4-miles/hr rate on level ground (5 6 MET) Go to 3 Class III
3. Can you carry at least 24 lb up 8 steps (10 MET)? Or can you a. Carry objects that weigh at least 80 lb (18 MET) b. Do outdoor work, shovel snow, spade soil (7 MET) c. Do recreational activities such as skiing, basketball, touch football, squash, handball (7 10 MET) d. Jog/walk 5 miles/h (9 MET) Class I Class II
MET, metabolic equivalents of activity.
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
15
Criteria for Determination of the Specific
Activity Scale Functional Class
Any Yes No
4. Can you shower without stopping (3.6 4.2 MET)? Or can you a. Strip and make bed (3.9 5 MET) b. Mop floors (4.2 MET) c. Hang washed clothes (4.4 MET) d. Clean windows (3.7 MET) e. Walk 2.5 miles/h (3 3.5 MET) f. Bowl (3 4.4 MET) g. Play golf, walk and carry clubs (4.5 MET) h. Push a power lawnmower (4 MET) Class III Go to 5
5. Can you dress without stopping because of symptoms (2 2.3 MET)? Class III Class IV
MET, metabolic equivalents of activity.
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
16
Angina
- Classified by symptom severity, disability,
specific activity scale - Number of vessels obstructed important
determinate of outcome - Risk factors for increased mortality
- heart failure
- smoking
- left main or left main equivalent CAD
- diabetes
- prior MI
17
Grading of Angina Pectoris by the Canadian
Cardiovascular Society Classification System
Class Description of Stage
Class I Ordinary physical activity does not cause angina, such as walking, climbing stairs. Angina occurs with strenuous, rapid, or prolonged exertion at work or recreation.
Class II Slight limitation or ordinary activity. Angina occurs on walking or climbing stairs rapidly, walking uphill, walking or stair climbing after meals, or in cold, or in wind, or under emotional stress, or only during the few hours after wakening. Walking more than 2 blocks on the level and climbing more than 1 flight of ordinary stairs at a normal pace and in normal condition.
Class III Marked limitations of ordinary physical activity. Angina occurs on walking 1 to 2 blocks on the level and climbing 1 flight of stairs in normal conditions and at a normal pace.
Class IV Inability to carry on any physical activity without discomfortanginal symptoms may be present at rest.
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
18
Etiology/Pathophysiology
- Coronary atherosclerotic plaque formation leads
to imbalance between O2 supply demand ?
myocardial ischemia - Ischemia lack of O2, decreased or no blood flow
in myocardium - Anoxia absence of O2 to myocardium
19
Etiology/Pathophysiology
- Determinants of myocardial oxygen demand (MVO2)
- HR
- contractility
- intramyocardial wall tension during systole (most
important) - Determinants of ischemia
- resistance in vessels delivering blood to
myocardium - MVO2
20
Etiology/Pathophysiology
- Coronary blood flow
- inversely related to arteriolar resistance
- directly related to coronary driving pressure
- Extent of functional obstruction important
limitation of coronary blood flow - severe stenosis (gt 70)
- ischemia symptoms at rest
20
21
(No Transcript)
22
Etiology/Pathophysiology
- Changes in O2 balance lead to rapid changes in
coronary blood flow - Mediators that affect O2 balance
- adenosine
- other nucleotides
- nitric oxide
- prostaglandins
- CO2
- H
22
23
Etiology/Pathophysiology
- Extrinsic factors
- alterations in intramyocardial wall tension
throughout the cardiac cycle - phasic systolic vascular bed compression
- factors that favor reduction in blood flow
- Intrinsic factors
- myogenic control
- Bayliss effect
- neural components
- parasympathetic nervous system, sympathetic
nervoussystem, coronary reflexes
23
24
Etiology/Pathophysiology
- Factors limiting coronary perfusion
- coronary reserve diminished at 85 obstruction
- critical stenosis occurs when obstructing lesion
encroaches on the luminal diameter exceeds 70
24
25
Short-Term Risk of Death or Nonfatal Myocardial
Infarction in Patients with Unstable Angina
Feature High Risk (At least 1 of the following features must be present) Intermediate Risk (No high-risk feature but must have 1 of the following) Low Risk (No high- or intermediate-risk feature but may have any of the following)
History Accelerating tempo of ischemic symptoms in preceding 48 h Prior Ml, peripheral or cerebrovascular disease, or CABG, prior aspirin use
Character of pain Prolonged ongoing (gt 20 min), rest pain Prolonged (gt 20 min), rest angina, now resolved, with moderate or high likelihood of CAD New-onset CCS class III or IV angina in the past 2 weeks without prolonged (gt 20 min) rest pain but with moderate or high likelihood of CAD
Clinical findings Pulmonary edema, most likely caused by ischemia New or worsening MR murmur S3 or new/worsening rales Hypotension, bradycardia, tachycardia Age gt 75 y
ECG Angina at rest with transient ST-segment changes gt 0.05 mV Bundle-branch block, new or presumed new T-wave inversions gt 0.2 mV Pathologic Q waves Normal or unchanged ECG during an episode of chest discomfort
Cardiac markers Markedly elevated (e.g., TnT or TnI gt 0.1 ng/mL) Slightly elevated (e.g., TnT gt 0.01 but lt 0.1 ng/mL) Normal
CABG, coronary artery bypass grafting CAD,
coronary artery disease CCS, Canadian
Cardiovascular Society ECG, electrocardiogram
Ml, myocardial infarction MR, mitral
regurgitation Tnl, troponin TnT, troponin T.
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
26
Clinical Presentation of Angina
- Many ischemia episodes are silent (no symptoms)
- Patients often have reproducible pattern, pain,
other symptoms - Increased frequency, severity, duration, symptoms
at rest suggests unstable angina
27
Clinical Presentation of Angina
- Symptoms
- sensation of pressure/burning over or near
sternum often but not always radiating - left jaw, shoulder, arm
- chest tightness, shortness of breath
- visceral pain lasts 0.5 to 30 min
- precipitating factors exercise, cold
environment, walking after a meal, emotional
upset, fright, anger, coitus - relief with rest, nitroglycerin
28
Clinical Presentation of Angina
- Signs
- abnormal precordial systolic bulge
- abnormal heart sounds
- Typically no abnormal laboratory tests
- Likely to have abnormal tests for IHD risk
factors - History of chest pain
29
Differential Diagnosis of Episodic Chest Pain
Resembling Angina Pectoris
Duration Quality Provocation Relief Location Comment
Effort angina 5 15 min Visceral (pressure) During effort or emotion Rest, NTG Substernal, radiates First episode vivid
Rest angina 5 15 min Visceral (pressure) Spontaneous (? with exercise) NTG Substernal, radiates Often nocturnal
Mitral prolapse Min hours Superficial (rarely visceral) Spontaneous (no pattern) Time Left anterior No pattern, variable
Esophageal reflux 10 min 1 h Visceral Spontaneous, cold liquids, exercise, lying down Foods, antacids, H2 blockers, proton pump inhibitors, NTG Substernal, radiates Mimics angina
Peptic ulcer Hours Visceral, burning Lack of food, "acid" foods Foods, antacids, H2 blockers, proton pump inhibitors Epigastric, substernal
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
30
Differential Diagnosis of Episodic Chest Pain
Resembling Angina Pectoris
Duration Quality Provocation Relief Location Comment
Biliary disease Hours Visceral (wax and wane) Spontaneous, food Time, analgesia Epigastric, radiates Colic
Cervical disk Variable (gradually subsides) Superficial Head and neck, movement and palpation Time, analgesia Arm, neck Not relieved by rest
Hyperventilation 2 3 min Visceral Emotion, tachypnea Stimulus removed Substernal Facial paraesthesia
Musculoskeletal Variable Superficial Movement, palpation Time, analgesia Multiple Tenderness
Pulmonary 30 min Visceral (pressure) Often spontaneous Rest, time broncho-dilator Substernal Dyspneic
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
31
Cardiac Findings in CAD Patients
Sign Clinical Significance Frequency
Abnormal precordial systolic bulge Left ventricular wall motion abnormality Not usually present unless patient has sustained a prior Ml (especially anterior wall) or is experiencing angina at time of examination
Decreased intensity of S1 Decrease in left ventricular contractility Difficult to evaluate in resting state, but can be commonly demonstrated during angina
Paradoxical splitting of S2 Left ventricular wall motion abnormality Very uncommon but occasionally noted during angina
S3 (ventricular gallop) Increased left ventricular diastolic pressure, with or without clinical CHF Not usually present unless patient sustained extensive Ml may occasionally be present during angina
S4 (atrial gallop) Reduced ventricular compliance ("stiff heart") Common very common in patients who have sustained a prior Ml as well as during angina
Apical systolic murmur (in absence of rheumatic mitral regurgitation or Barlow syndrome) Papillary muscle dysfunction Not usually present unless patient has sustained prior Ml
Diastolic murmur (in absence of aortic regurgitation) Coronary artery stenosis Rare
CHF, congestive heart failure MI, myocardial
infarction S1, first heart sound S2, second
heart sound S3, third heart sound S4, fourth
heart sound
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
32
(No Transcript)
33
Diagnostic Tests
- Electrocardiogram (ECG)
- normal in ½ of patients with angina not
experiencing an acute attack - ST-T wave changes
- depression
- T-wave inversion
- ST-segment elevation
- significant ischemia
- ST-segment depression gt 2 mm
- exertional hypotension
- reduced exercise tolerance
34
Lead V4 at rest (top) and after 4½ min of
exercise (bottom). There is 3 mm (0.3 mV) of
horizontal ST-segment depression, indicating a
positive test for ischemia.
35
Diagnostic Tests
- Exercise Tolerance Testing (ETT)
- recommended for patients with intermediate
pretest probability of CAD based on age, gender,
symptoms - insensitive for predicting coronary artery
anatomy but correlates well with outcome - Echocardiography
- useful if physical examination suggests valvular,
pericardial disease, ventricular dysfunction
36
45-year-old avid jogger who began experiencing
classic substernal chest pressure underwent an
exercise echo study. With exercise the patient's
heart rate increased from 52 to 153 bpm. The left
ventricular chamber dilated with exercise, and
the septal and apical portions became akinetic to
dyskinetic (red arrow). These findings are
strongly suggestive of a significant flow
limiting stenosis in the proximal left anterior
descending coronary artery, which was confirmed
at coronary angiography.
37
Diagnostic Tests
- Cardiac imaging
- radionucleotide angiocardiography
- technetium pyrophosphate scans
- positron emission tomography
- ultrarapid computerized tomography
- spiral CT
- ultrafast CT
- electron-beam CT
- Cardiac catheterization angiography
38
Stress and rest myocardial perfusion PET images
obtained with rubidium-82 in a patient with chest
pain on exertion. The images demonstrate a large
and severe stress perfusion defect involving the
mid and apical anterior, anterolateral, and
anteroseptal walls, and the LV apex, showing
complete reversibility, consistent with extensive
and severe ischemia in the mid left anterior
descending coronary artery territory (red
arrows).
39
(No Transcript)
40
(No Transcript)
41
IHD Treatment
- Short term goals
- reduce/prevent angina symptoms that limit
exercise capability impair quality of life
(QOL) - Long-term goals
- prevent CHD events
- MI
- arrhythmias
- heart failure
- extend the patients life
42
(No Transcript)
43
IHD Treatment
- Risk factor identification/modification
- risk factors play a major role in determining
occurrence severity of IHD - risk factors are additive
- classified as alterable or unalterable
44
IHD Treatment
- Unalterable risk factors
- gender
- age
- family history
- environmental influences
- climate, air pollution, trace metals in drinking
water - diabetes mellitus
45
IHD Treatment
- Alterable risk factors
- smoking
- HTN
- hyperlipidemia
- obesity, sedentary lifestyle
- hyperuricemia
- psychosocial factors (stress, type A behavior)
- medications
- progestins
- corticosteroids
- cyclosporine
46
The American College of Cardiology and American
Heart Association Evidence Grading System
Recommendation Class Recommendation Class Level of Evidence Level of Evidence
I Conditions for which there is evidence or general agreement that a given procedure or treatment is useful and effective A Data derived from multiple randomized clinical trials with large numbers of patients
II Conditions for which there is conflicting evidence or a divergence of opinion about the usefulness/efficacy of a given procedure or treatment is useful and effective B Data derived from a limited number of randomized trials with small numbers of patients, careful analyses of nonrandomized studies, or observational registries
IIa Weight of evidence/opinion is in favor or usefulness/efficacy C Expert consensus was the primary basis for the recommendation
IIb Usefulness/efficacy is less-well established by evidence/opinion
III Conditions for which there is evidence or general agreement that a given procedure or treatment is not useful/effective and in some cases may be harmful
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
47
Stable Exertional Angina Pectoris
- ASA (Class I, Level A)
- ß-blockers with prior MI (Class I, Level A)
- ACE inhibitors for patients with CAD diabetes
or LV systolic dysfunction (Class I, Level A) - LDL-lowering therapy with CAD LDL gt 130 mg/dL
(Class I, Level A) - target LDL lt 100 mg/dL
- lt 70 mg/dL in patients with CHD multiple risk
factors - Sublingual nitroglycerin for immediate angina
relief (Class I, Level B)
48
Stable Exertional Angina Pectoris
- Calcium antagonists or long-acting nitrates for
symptom reduction when ß-blockers contraindicated
(Class I, Level B) - Calcium antagonists or long-acting nitrates in
combination with ß-blockers when initial
ß-blocker treatment is inadequate (Class I, Level
C) - Calcium antagonists or long-acting nitrates as
substitutes for ß-blockers if initial ß-blocker
treatment leads to intolerable side effects
(Class I, Level A)
49
Stable Exertional Angina Pectoris
- May substitute clopidogrel when ASA
contraindicated (Class IIa, Level B) - Use of long-acting nondihydropyridine calcium
antagonists instead of ß-blockers as initial
therapy (Class IIa, Level B) - Therapies to avoid
- dipyridamole (Class III, Level B)
- chelation therapy (Class III, Level B)
50
Effect of Drug Therapy on Myocardial O2 Demand
LV Wall Tension LV Wall Tension
Heart Rate Myocardial Contractility Systolic Pressure LV Volume
Nitrates ? 0 ? ??
ß-Blockers ?? ? ? ?
Nifedipine ? 0 or ? ?? 0 or ?
Verapamil ? ? ? 0 or ?
Diltiazem ?? 0 or ? ? 0 or ?
Calcium channel antagonists and nitrates also may increase myocardial oxygen supply through coronary vasodilation. Diastolic function may be improved with verapamil, nifedipine, and perhaps, diltiazem. These effects may vary from those indicated in the table depending on individual patient baseline hemodynamics.
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
51
Stable Exertional Angina Pectoris
- ß-blocker place in therapy
- effective in chronic exertional angina as
monotherapy and in combo with nitrates and/or
CCBs - 1st line in chronic angina that requires daily
maintenance therapy - ideal candidates
- physical activity figures prominently in anginal
attacks - coexistent hypertension
- history of supraventricular arrhythmias or
post-MI angina - anxiety associated with angina
52
Stable Exertional Angina Pectoris
- ß-blockers
- symptom control
- reduce risk of recurrent MI, CAD mortality
- may be used for chronic prophylaxis in patients
with gt 1 angina episodes/day - smokers have reduced anti-anginal efficacy
- some have reduced efficacy based on lipid
solubility - propranolol lipid soluble, inducible metabolism
53
Stable Exertional Angina Pectoris
- ß-blockers
- overall effect of ß-blockers in patients with
effort-induced angina ? reduction in O2 demand - do not improve O2 supply
- can blunt reflex tachycardia from nitrate therapy
- may decrease exercise capacity in healthy
individuals or those with HTN - may improve exercise tolerance in angina patients
54
Stable Exertional Angina Pectoris
- ß-blockers
- dosing based on t½
- disparity between t½ duration of action for
several BBs - renal/hepatic dysfunction affect disposition
- route of elimination not major consideration in
drug selection
55
Stable Exertional Angina Pectoris
- ß-blocker adverse effects
- abrupt withdrawal associated with increased
severity number of pain episodes myocardial
infarction - pharmacologic effects
- CNS effects
- fatigue
- malaise
- depression
- hypotension
- decompensated heart failure
- bradycardia
- heart block
- bronchospasm
- altered glucose metabolism
56
Stable Exertional Angina Pectoris
- Nitrate place in therapy
- terminate acute anginal attack
- prevent effort/stress-induced attacks
- long-term prophylaxis
- usually in combination with ß-blockers or CCBs
- formulations
- chewable
- oral
- transdermal
- ointments
- spray
- IV
57
Stable Exertional Angina Pectoris
- Nitrate therapy for acute attacks
- sublingual
- buccal
- spray products
- Symptom prophylaxis when undertaking activities
that precipitate attacks - oral or transdermal products
- 0.3 to 0.4 mg SL 5 min prior to activity
- Chronic prophylaxis with long-acting forms
- tolerance limiting factor
58
Stable Exertional Angina Pectoris
- Nitrate therapy
- reduces MVO2 2? to venodilation
arterial-arteriolar dilation ? reduction in wall
stress from reduced ventricular volume pressure - systemic venodilation increases flow to deep
myocardial tissue - dilation of large small intramural coronary
arteries, collateral dilation, coronary artery
stenosis dilation, abolition of normal tone in
narrowed vessels, relief of spasms
59
Stable Exertional Angina Pectoris
- Nitrate therapy
- large 1st-pass effect
- short t½ (except isosorbide mononitrate)
- see Nitrate Products chart on slide 61
- large volume of distribution
- high clearance rates
- large interindividual variation in plasma/blood
concentrations - saturable metabolism
- accumulation of metabolites with multiple doses
- drug adsorption to PVC tubing, syringes
60
Stable Exertional Angina Pectoris
- Nitrate therapy adverse effects
- extension of pharmacologic effects
- postural hypotension with CNS symptoms,
headaches, flushing 2? to vasodilation - occasional nausea from smooth muscle relaxation
- reflex tachycardia, but bradycardia has been
reported - rash with all products (particularly with
patches) - production of methemoglobinemia with high doses
for extended periods - measurable ethanol propylene glycol
concentrations with IV nitroglycerin - tolerance
61
Nitrate Products
Product Onset (min) Duration Initial Dose
Nitroglycerin IV Sublingual/lingual Oral Ointment Patch 1 2 1 3 40 20 60 40 60 3 5 min 30 60 min 3 6 h 2 8 h gt 8 h 5 mcg/min 0.3 mg 2.5 9 mg tid 0.5 1 in 1 patch
Erythritol tetranitrate 5 30 4 6 h 5 10 mg tid
Pentaerythritol tetranitrate 30 4 8 h 10 20 mg tid
Isosorbide dinitrate Sublingual/chewable Oral 2 5 20 40 1 2 h 4 6 h 2.5 5 mg tid 5 20 mg tid
Isosorbide mononitrate 30 60 6 8 h 20 mg daily, bida
a Product dependent
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
62
Stable Exertional Angina Pectoris
- Calcium channel blockers (CCBs)
- effective monotherapy (usually used if patients
are intolerant of ß-blockers) - generally used in combination with ß-blockers
- improve coronary blood flow through coronary
artery vasodilation, decrease MVO2 - provide better skeletal muscle oxygenation than
ß-blockers ? decrease fatigue, improve exercise
tolerance - CCBs have similar efficacy
- differences in electrophysiology,
peripheral/central hemodynamic effects, ADR
profiles useful in selecting appropriate agent
63
Stable Exertional Angina Pectoris
- Calcium channel blockers (CCBs)
- ideal candidates
- contraindications/intolerance to ß-blockers
- coeixting conduction system disease (except
verapamil, diltiazem) - Prinzmetal angina
- peripheral vascular disease
- severe ventricular dysfunction (amlodipine drug
of choice) - concurrent HTN
64
Stable Exertional Angina Pectoris
- Calcium channel blockers (CCBs)
- vasodilation of systemic arterioles coronary
arteries - reduction of arterial pressure and coronary
vascular resistance - depression of myocardial contractility
conduction velocity of the SA/AV nodes - MVO2 reduction due to reduced wall tension 2? to
reduced arterial pressure - may improve coronary blood flow through areas of
fixed coronary obstruction - inhibits coronary artery vasomotion/vasospasm
- non-dihydropyridine products affect AV conduction
and contractility
65
Stable Exertional Angina Pectoris
- Calcium channel blockers (CCBs)
- large, variable, 1st-pass metabolism
- 20 to 50 bioavailability for diltiazem,
nicardipine, nifedipine, verapamil, felodipine,
isradipine - amlodipine bioavailability 60 to 80
- most CCBs eliminated via CYP 3A4 other CYP
isoenzymes
66
Stable Exertional Angina Pectoris
- Ranolazine
- reduces Ca2 overload in ischemic myocytes
through selective inhibition of late Na current
(INa) - does not affect HR, inotropic state, hemodynamic
state or increase coronary blood flow - indicated for chronic angina treatment
- prolongs QT interval
- reserved for patients who have not achieved
adequate response with other antianginal agents
67
Stable Exertional Angina Pectoris
- Ranolazine
- dose 500 mg BID then 1000 mg BID
- contraindications
- preexisting QT interval prolongation
- hepatic impairment
- drug interactions
- other QT interval-prolonging medications
- cytochrome P450 3A inhibitors decrease ranolazine
clearance
68
Clinical Controversy
- MERLIN-TIMI 36
- Metabolic Efficiency With Ranolazine for Less
Ischemia in Non-ST-Elevation Acute Coronary
Syndromes - Randomized, double-blind, controlled trial
(n6560) - 2 groups
- ranolazine 1000 mg BID
- placebo
Morrow DA, Scirica BM, Karwatowska-Prokopczuk E,
et al. Effects of ranolazine on recurrent
cardiovascular events in patients with
non-ST-elevation acute coronary syndromes the
MERLIN TIMI 36 randomized trial. JAMA
20072971775 83.
Evaluation of the Glycometabolic Effects of
Ranolazine in Patients With and Without Diabetes
Mellitus in the MERLIN-TIMI 36 Randomized
Controlled Trial Circulation, 2009 119 2032 -
2039.
69
Clinical Controversy
- MERLIN-TIMI 36 results
- NSTEMI angina symptom relief
- 6.2 HbA1c reduction at 4 months ranolazine
group - 5.9 HbA1c reduction at 4 months placebo
- 0.30 versus 0.04 (plt0.001) clinical
significance? - no significant reduction in composite 1 outcome
at (median follow-up 348 days) - CV death
- MI, recurrent ischemia
Morrow DA, Scirica BM, Karwatowska-Prokopczuk E,
et al. Effects of ranolazine on recurrent
cardiovascular events in patients with
non-ST-elevation acute coronary syndromes the
MERLIN TIMI 36 randomized trial. JAMA
20072971775 83.
Evaluation of the Glycometabolic Effects of
Ranolazine in Patients With and Without Diabetes
Mellitus in the MERLIN-TIMI 36 Randomized
Controlled Trial Circulation, 2009 119 2032 -
2039.
70
(No Transcript)
71
(No Transcript)
72
Stable Exertional Angina Pectoris
- Nonpharmacologic therapy
- revascularization
- coronary artery bypass grafting
- percutaneous transluminal coronary angioplasty
73
Recommended Mode of Coronary Revascularization
Extent of Disease Treatment Class/Level of Evidence
Left main disease,a candidate for CABG CABG PCI I/A III/C
Left main disease, not a candidate for CABG PCI IIb/C
Three-vessel disease with EF lt 0.50 CABG I/A
Multivessel disease including proximal LAD with EF CABG I/A
lt 0.50 or treated diabetes PCI IIb/B
Multivessel disease with EF gt 0.50 and without diabetes PCI I/A
One- or two-vessel disease without proximal LAD but with large areas of myocardial ischemia or high-risk criteria on noninvasive testing CABG or PCI I/B
One-vessel disease with proximal LAD CBAG or PCI IIa/B
One- or two-vessel disease without proximal LAD with small area of ischemia or no ischemia on noninvasive testing CABG or PCI III/C
Insignificant coronary stenosis CABG or PCI III/C
CABG, coronary artery bypass grafting EF,
ejection fraction LAD, left anterior descending
coronary artery PCI, percutaneous coronary
intervention. a50 diameter stenosis
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
74
(No Transcript)
75
Stable Exertional Angina Pectoris
- Revascularization
- based on extent of coronary disease ( of
vessels, location/amount of stenosis)
ventricular function - complications coronary artery spasm,
intraluminal thrombus - combination therapy with acetylsalicylic acid,
unfractionated heparin, or low-molecular-weight
heparin, glycoprotein IIb/IIIa receptor
antagonists stents have reduced occurrence of
reocclusion late restenosis
76
Stable Exertional Angina Pectoris
- Coronary artery bypass grafting (CABG)
- reduces symptomatic angina not controlled by
medical management or PCI - improves patient lifestyle
- reduces CAD mortality
- reduces need for nitrates, ß-blockers
77
Stable Exertional Angina Pectoris
- Percutaneous transluminal coronary angioplasty
(PTCA) - reduced stenosis due to
- compression, redistribution of plaque
- embolization of plaque contents
- aneurysm formation
- disruption of plaque arterial wall
- patients usually heparinized during PTCA to
prevent immediate thrombus formation at site of
arterial injury - anticoagulation up to 24 hrs
78
Stable Exertional Angina Pectoris
- Percutaneous transluminal coronary angioplasty
(PTCA) - prevention of restenosis
- combination therapy with acetylsalicylic acid,
heparin, GP IIa/IIIa receptor antagonists - bivalirudin
- drug-eluting bare metal stents
79
Stable Exertional Angina Pectoris
- PTCA vs CABG
- low-risk patients have greater alleviation of
symptoms with PTCA - moderate-risk patients had equal mortality MI
rates with PTCA or CABG - high-risk patients showed improved survival with
CABG than medical therapy
80
Stable Exertional Angina Pectoris
- Drug-eluting stents
- sirolimus (Cypher)
- paclitaxel (Taxus)
- zotarolimus (Endeavor)
- target revascularization needed less often than
bare stents - combination antiplatelet therapy (ASA
clopidogrel) for gt 1 yr following implantation
Eisenberg MJ Richard PR, BSc Libersan D Filion
KB. Safety of Short-Term Discontinuation of
Antiplatelet Therapy in Patients With
Drug-Eluting Stents. Circulation. 2009 119
1634-1642.
81
Drug-eluting stents
- Antiplatelet therapy often discontinued in
surgical patients with drug-eluting stents - risk factor for late stent thrombosis
- Medline search for late very late stent
thrombosis cases Jan 2001 to July 2008 - When patients stopped antiplatelet agents
simultaneously, median time to event 7 days - If the thienopyridine was stopped ASA
continued, median time to event 122 days
Eisenberg MJ Richard PR, BSc Libersan D Filion
KB. Safety of Short-Term Discontinuation of
Antiplatelet Therapy in Patients With
Drug-Eluting Stents. Circulation. 2009 119
1634-1642.
82
Variant Angina Pectoris
- Prinzmetal angina
- associated with ST-segment elevation
- commonly resolves without progression to MI
- usually younger patients
83
Variant Angina Pectoris
- Causes
- imbalance between endothelium-produced
vasodilator factors (prostacyclin, nitric oxide)
vasoconstrictor factors (endothelin,
angiotensin II) - imbalance of autonomic control characterized by
parasympathetic dominance of inflammation - adrenoreceptor polymorphisms may predispose
patients to developing vasospasm
84
Variant Angina Pectoris
- Precipitating factors
- hyperventilation
- exercise
- exposure to cold
- May have no apparent precipitating cause
85
Coronary Artery Spasm
- Diagnosis
- ST-segment elevation during transient chest
discomfort (usually at rest) that resolves when
chest discomfort diminishes in patients with
normal or non-obstructive lesions - In absence of ST-segment elevation, may use
provocative tests to precipitate coronary artery
spasm - ergonovine, acetylcholine, methacholine
- withdraw nitrates CCB prior to testing
86
Coronary Artery Spasm
- Treatment
- optimization of therapy includes dose titration
- treat all patients for acute attacks
- maintain prophylactic treatment 6 to 12 months
following initial episode - eliminate aggravating factors
- alcohol
- cocaine
- cigarette smoking
87
Coronary Artery Spasm
- Treatment
- nitrates for acute attacks
- CCBs
- nifedipine, verapamil, diltiazem equally
effective single agents for initial treatment - dose titration needed
- combination therapy with nifedipine-diltiazem or
nifedipine-verapamil useful for patients
unresponsive to single-drug regimens - ß-blockers have little or no role
88
Silent Ischemia
- Associated with ST-segment elevation, depression
- Frequently occurs without antecedent HR, BP
changes - ischemia from reduction in O2 supply
- 2 classes
- Class I patients do not experience angina
- Class II patients have both asymptomatic
symptomatic ischemia - Associated with reduced survival, increased need
for PTCA/CABG, increased risk of acute MI
89
Silent Ischemia
- Causes
- increased physical activity
- sympathetic nervous system activation
- ? cortisol secretion
- ? coronary artery tone
- enhanced platelet aggregation due to endothelial
dysfunction leading to intermittent coronary
obstruction
90
Silent Ischemia
- Diagnosis ambulatory ECG
- Initial management
- modify IHD risk factors
- HTN
- hypercholesterolemia
- smoking
- Treatment goal
- reduce number of ischemic episodes (symptomatic
asymptomatic), regardless of direction of
ST-segment shift
91
Silent Ischemia
- Pharmacologic treatment
- ß-blockers
- most useful for post-MI patients or those with
high level of sympathetic nervous system activity - CCBs alone or in combination effective in
reducing symptomatic asymptomatic ischemia - do not interrupt diurnal surge in ischemia
- less effective than ß-blockers
- combination ß-blockers CCBs better response
than CCBs nitrates or CCB monotherapy
92
Therapeutic Outcomes
- Angina symptom improvement
- Improved cardiac performance
- Risk factor reduction
- Increased exercise capacity
- May use coronary angiography to assess extent of
stenosis or restenosis after angioplasty or CABG
93
Clinical Controversy
- Many long-term trials compare ß-blockade vs CCBs
to determine superior survival benefit - ß-blockers recommended 1st line prophylactic
therapy for symptomatic angina patients requiring
daily pharmacologic therapy - effective in post-MI patients
- favorable adverse effect profile
- Stable CAD medical management produces outcomes
similar to revascularization - may impact future use of healthcare resources
94
Clinical Controversy
- Recent developments in understanding organic
nitrates bioactivation raise concern over
endothelial dysfunction induced by long-term
nitrate administration - Nitrate products activated via different
mechanisms - impacts long-term effectiveness of individual
drugs
95
American College of Cardiology, American Heart
Association, and Physician Consortium for
Performance Improvement Chronic Stable Coronary
Artery Disease Core Physician Performance
Measurement Seta
Clinical Recommendations
Blood pressure measurement A blood pressure ready is recommended at every visit. Recommended blood pressure management targets are 130 mm Hg systolic (Class I Recommendation, Level A Evidence) and 85 mm Hg diastolic in patient with CAD coexisting condition (e.g., diabetes, heart failure, or renal failure) and lt140/90 mm Hg in patient with CAD and no coexisting condition.
Lipid profile A lipid profile is recommended and should include total cholesterol, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), and triglycerides. (Class I Recommendation, Level C Evidence)
Symptom and activity assessment Regular assessment of patients' anginal symptoms and levels of activity is recommended. (Serves as a basis for treatment modification.)
Smoking cessation Smoking status should be determined and smoking cessation counseling and interventions are recommended. (Class I Recommendation, Level B Evidence)
Screening for diabetes Denominator exclusion patients with documented DM Screening for diabetes is recommended in patients who are considered high risk (e.g., CAD) (Class I Recommendation, Level A Evidence)
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
96
American College of Cardiology, American Heart
Association, and Physician Consortium for
Performance Improvement Chronic Stable Coronary
Artery Disease Core Physician Performance
Measurement Seta
Clinical Recommendations
Antiplatelet therapy Denominator exclusion Documentation of medical reason(s)b for not prescribing antiplatelet therapy documentation of patient reason(s)c for not prescribing antiplatelet therapy Routine use of aspirin is recommended in the absence of contraindications. If contraindications exist, other antiplatelet therapies may be substituted. (Class I Recommendation, Level A Evidence)
ACE inhibitor therapy Denominator inclusion Patient with CAD who also has diabetes and/or left ventricular systolic dysfunction (LVSD) (left ventricular ejection fraction LVEF lt 40 or moderately or severely depressed left ventricular systolic function) Denominator exclusion Documentation that ACE inhibitor was not indicated (e.g., patients on angiotensin receptor blockers ARB) documentation of medical reason(s)b for not prescribing ACE inhibitor documentation of patient reason(s)c for not prescribing ACE inhibitor ACE inhibitor use is recommended in all patients with CAD who also have diabetes and/or LVSD (Class I Recommendation, Level A Evidence) ACE inhibitor use is also recommended in patients with CAD or other vascular disease (Class IIa Recommendation, Level B Evidence)
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
97
American College of Cardiology, American Heart
Association, and Physician Consortium for
Performance Improvement Chronic Stable Coronary
Artery Disease Core Physician Performance
Measurement Seta
Clinical Recommendations
ß-Blocker therapyprior myocardial infarction (MI) Denominator inclusion Prior MI Denominator exclusion Documentation that a ß-blocker was not indicated documentation of medical reason(s)b for not prescribing a ß-blocker documentation of patient reason(s)c for not prescribing a ß-blocker ß-Blocker therapy is recommended for all patients with prior MI in the absence of contraindications. (Class I Recommendation, Level A Evidence)
Drug therapy for lowering LCL-cholesterol Denominator exclusion Documentation that a statin was not indicatede documentation of medical reason(s)b for not prescribing a statin documentation of patient reason(s)c for not prescribing statin The LCL-C treatment goal is lt100 mg/dL. Persons with established coronary heart disease (CHD) who have a baseline LCL-C 130 mg/dL should be started on a cholesterol-lowering drug simultaneously with therapeutic lifestyle changes and control of nonlipid risk factors. (Class I Recommendation, Level A Evidence)
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
98
Table Footnotes
- aRefers to all patients diagnosed with CAD
- bMedical reasons for not prescribing antiplatelet
therapy (aspirin, clopidogrel, or combination of
aspirin and dipyridamole) active bleeding in the
previous 6 months with required hospitalization
and/or transfusion(s), patient on other
antiplately therapy, etc. - Medical reasons for not prescribing a statin
clinical judgement, documented LCL-C lt 130 mg/dL,
etc. - Medical reasons for not prescribing a ß-blocker
bradycardia (defined as heart rate lt 50 beats/min
without ß-blocker therapy), history of class IV
(congestive) heart failure, history of second- or
third-degree atrioventricular block without
permanent pacemaker, etc. - Medical reasons for not prescribing ACE inhibitor
(ACEI) allergy, angioedema caused by ACEI,
anuric rental failure caused by ACEI, pregnancy,
moderate or severe aortic stenosis, etc. - cPatient reasons for not prescribing antiplatelet
therapy, statin, -blocker, or ACEI economic,
social, and/or religious, etc. - dAntiplatelet therapy may include aspirin,
clopidogrel, or combination of aspirin and
dipyridamole. - eNot indicated for a statin refers to LCL-C lt 100
mg/dL. - fTest measure.
- gScreening for diabetes is usually done by
fasting blood glucose or 2-hour glucose tolerance
testing. Clinical recommendations indicate
screening should be considered at 3-year
intervals.
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
99
Acknowledgements
- Prepared By Amy Pai, Pharm.D.
- Series Editor April Casselman, Pharm.D.
- Editor-in-Chief Robert L. Talbert, Pharm.D.,
FCCP, BCPS, FAHA - Chapter Author/Section Editor
- Robert L. Talbert, Pharm.D., FCCP, BCPS, FAHA