
Newborn Screening via Tandem Mass Spectrometry, Michigan, 2006 - PowerPoint PPT Presentation
1 / 1
Title:
Newborn Screening via Tandem Mass Spectrometry, Michigan, 2006
Description:
Glutaric Acidemia Type II- (GA II) 0. 0.01. 0. 15 (40.0) ... Glutaric Acidemia Type I (GA I) 2.7. 0.029. 1 : 125,600. 1. 37 (16.2) ... – PowerPoint PPT presentation
Number of Views:162
Avg rating:3.0/5.0
Title: Newborn Screening via Tandem Mass Spectrometry, Michigan, 2006
1
Newborn Screening via Tandem Mass Spectrometry,
Michigan, 2006
Steven Korzeniewski, MS, MA, William Young, PhD,
and Violanda Grigorescu, MD, MSPH, Michigan
Department of Community Health, Division of
Genomics, Perinatal Health and Chronic Disease
Epidemiology
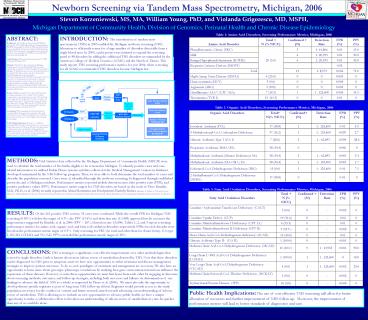
Table 1 Amino Acid Disorders, Screening
Performance Metrics, Michigan, 2006
ABSTRACT Background Since tandem mass
spectrometry (TMS) was introduced in 2003, the
Michigan Newborn Screening Program (MI NBS) has
expanded to include 41 TMS detectable disorders
as recommended by the American College of Medical
Genetics (ACMG). This study reports screening
performance metrics for year 2006, when screening
for all ACMG recommended TMS disorders became
Michigan law. Study Question What are the
performance metrics for TMS screening in
Michigan, 2006? Methods Vital Statistics data
collected by the Michigan Department of Community
Health (MDCH) were used to calculate the total
number of live births eligible to be screened in
Michigan. To identify positive cases and
case-related information we utilized Perkin Elmer
systems and data collected at the Medical
Management Centers in databases
developed/maintained by the NBS follow-up
program. Thus, we were able to both determine the
total number of cases and describe the population
screened. Cases were a) identified through the
newborn screening, b) diagnosed through
established protocols, and c) Michigan residents.
Performance metrics reported include detection
rates, false positive rates, and positive
predictive values. Results MI NBS screened
99.6 of the 126,509 live births occurring in
Michigan in 2006. Overall, 10.8 of infants
screened were in neonatal intensive care units,
1.4 were born with a weight less than 1500g, and
0.6 were born prior to 28 weeks gestational age.
Of the 261 positive screens, 35 infants were
diagnosed as having a TMS disorder. The TMS
disorder detection rate was 1 3,589, the
positive predictive value was 13.4, and the
false positive rate was 0.18. Conclusions TMS
screening has revolutionized newborn screening.
The performance metrics measured in this study
indicate that the use of TMS is a significant and
cost-effective improvement over the use of other
single disorder screening methodologies. Public
Health Implications The use of cost effective
screening (TMS) will allow for better allocation
of resources and further improvement of
follow-up. Moreover, the improvement of
performance metrics would lead to better
standards of diagnostics and care. Little is
known about TMS disorders and so we must also
take the opportunity to develop disease specific
registries as part of long term follow-up efforts.
INTRODUCTION The introduction of tandem mass
spectrometry (TMS) in 2003 enabled the Michigan
newborn screening (NBS) laboratory to efficiently
screen for a large number of disorders detectable
from a single blood spot. In 2005, a pilot
project was initiated to expand the screening
panel to 48 disorders by adding the additional
TMS disorders recommended by the American College
of Medical Genetics (ACMG) and the March of
Dimes. This study reports TMS screening
performance metrics for year 2006, when screening
for all ACMG recommended TMS disorders became
Michigan law.
Amino Acid Disorder Total N ( NICU) Confirmed (N) Detection Rate FPR () PPV ()
Phenylketonuria -Classic (PKU) 20 (5.0) 3 1 41,866 0.01 15.0
Mild 20 (5.0) 6 1 20,933 0.01 30.0
Benign Hypephenyla-laninemia (H-PHE) 20 (5.0) 6 1 20,933 0.01 30.0
Biopterin Cofactor Defects (BIOPT) 20 (5.0) - - 0.02 -
Total 20 (5.0) 15 1 8,373 0.004 75.0
Maple Syrup Urine Disease (MSUD) 4 (25.0) 0 0 0.003 0
Homocystinuria (HCY) 5 (0.0) 0 0 0.004 0
Arginemia (ARG) 3 (100) 0 0 0.002 0
Citrullinemia/ASA (CIT/ASA) 7 (14.3) 1 1 125,600 0.005 14.3
Tyrosinemia (TYR I) 13 (61.5) 0 0 0.01 0
Table 2 Organic Acid Disorders, Screening
Performance Metrics, Michigan, 2006
Organic Acid Disorders Total N( NICU) Confirmed (N) Detection Rate FPR () PPV ()
Isovaleric Acidemia (IVA) 17 (58.8) 1 1 125,600 0.01 5.9
3-Methylcrotonyl-CoA Carboxylase Deficiency 37 (16.2) 1 1 125,600 0.029 2.7
Glutaric Acidemia Type I (GA I) 7 (28.6) 2 1 62,893 0.004 28.6
Proprionic Acidemia/MMA (PA) 58 (34.4) 0 - 0.046 0
Methylmalonic Acidemia (Mutase Deficiency) MA 58 (34.4) 2 1 62,893 0.045 3.4
Methylmalonic Acidemia (MA-Cbl C, D) 58 (34.4) 1 1 125,600 0.045 1.7
Isobutyryl-CoA Dehydrogenase Deficiency (IBG) 15 (0.0) 1 1 125,600 0.01 7.1
2-Methylbutyryl-CoA Dehydrogenase Deficiency (2MBG) 17 (58.8) 0 - 0.01 0
Figure 1 Overview of the Michigan Newborn
Screening Program
METHODS Vital Statistics data collected by the
Michigan Department of Community Health (MDCH)
were used to calculate the total number of live
births eligible to be screened in Michigan. To
identify positive cases and case-related
information we utilized Perkin Elmer systems and
data collected at the Medical Management Centers
in databases developed/maintained by the NBS
follow-up program. Thus, we were able to both
determine the total number of cases and describe
the population screened. Cases were a)
identified through the newborn screening, b)
diagnosed through established protocols, and c)
Michigan residents. Performance metrics reported
include detection rates, false positive rates
(FPR), and positive predictive values (PPV).
Performance metric targets for TMS disorders are
based on the work of Piero Rinaldo, M.D., Ph.D.,
et al. (2006) recently reported in Mental
Retardation and Developmental Disability Reviews.
(Rinaldo, P., Zafari, S., Tortorelli, S., and
Matern, D. (2006) Making The Case for Objective
Performance Metrics In Newborn Screening by
Tandem Mass Spectrometry. Mental Retardation and
Developmental Disabilities Research Reviews. 12
255-261.)
Table 3 Fatty Acid Oxidation Disorders,
Screening Performance Metrics, Michigan, 2006
Fatty Acid Oxidation Disorders Total N ( NICU) Confirmed (N) Detection Rate FPR () PPV ()
Carnitine/Acylcarnitine Translocase Deficiency- (CACT) 3 (0.0) 0 - 0.002 0
Carnitine Uptake Defect- (CUP) 19 (31.6) 0 - 0.02 0
Carnitine Palmitoyltransferase I Deficiency- (CPT 1A) 6 (33.3) 0 - 0.01 0
Carnitine Palmitoyltransferase II Deficiency-(CPT II) 3 (33.3 ) 0 - 0.002 0
Short-Chain Acyl-CoA Dehydrogenase deficiency- (SCAD) 15 (40.0) 0 - 0.01 0
Glutaric Acidemia Type II- (GA II) 1 (100.0) 0 - 0.001 0
Medium-Chain Acyl-CoA Dehydrogenase Deficiency- (MCAD) 10 (10.0 ) 9 1 13,955 0.001 90.0
Long-Chain L-30H Acyl-CoA Dehydrogenase Deficiency- (LCHAD) 1 (100.0) 1 1 125,600 0 100
Very Long-Chain Acyl-CoA Dehydrogenase Deficiency-(VLCAD) 4 (0.0) 1 1 125,600 0.002 25.0
Medium-Chain Ketoacyl-CoA Thiolase Deficiency- (MCKAT) 3 (0.0) 0 - 0.002 0
Tryfunctional Protein Disease- (TFP) 10 (0.0) 0 - 0.008 0
RESULTS Of the 261 positive TMS screens, 35
cases were confirmed. While the overall FPR for
Michigan TMS screening (0.18) is below the
target of 0.3, the PPV (13.4) and detection
rate (13,589) approach but do not meet the
target metrics suggested by Rinaldo, et al. in
2006 (PPV gt 20, Detection rate 13,000). Tables
1, 2, and 3 report screening performance metrics
for amino acid, organic acid, and fatty acid
oxidation disorders respectively. FPRs for each
disorder were less than the performance metric
target of 0.3. Only screening for PKU (in total
and other than for classic form), GA type I,
MCAD, LCHAD, and VLCAD PPVs exceeded the
performance metric target of 20.
CONCLUSIONS TMS screening is a significant,
cost-effective improvement over other
methodologies that screen for single disorders.
Little is known about most inborn errors of
metabolism detected by TMS. Now that these
disorders can be diagnosed via NBS prior to
symptom onset we have new opportunities to refine
treatment and disease management strategies to
improve patient outcomes. To do so, new paradigms
of treatment and management are necessary. We
also have an opportunity to learn more about
genotype/phenotype correlations by studying how
gene environment interactions influence the
expression of these diseases. However, to seize
these opportunities we must first learn from each
other by engaging in discourse about screening
methods, outcomes, and follow-up strategies,
including both successes and failures via
dissemination of our findings to advance the
field of NBS as a whole as requested by Pierro et
al. (2006). We must also take the opportunity to
develop disease specific registries as part of
long term NBS follow-up efforts. Registries would
provide access to the study population necessary
for the conduct of current and future research
aimed towards advancing our understanding of
inborn errors of metabolism. TMS is allowing us
to embark on new opportunities to advance public
health, we have a unique opportunity to make a
collaborative effort to broaden our understanding
of inborn errors of metabolism at a rate far
quicker than any of us could do alone.
Public Health Implications The use of cost
effective TMS screening will allow for better
allocation of resources and further improvement
of NBS follow-up. Moreover, the improvement of
performance metrics will lead to better standards
of diagnostics and care.
Recommended
CrystalGraphics Presentations





























