
Malaria in Pakistan - PowerPoint PPT Presentation
1 / 8
Title:
Malaria in Pakistan
Description:
M. Naeem Durrani, Technical Advisor HealthNet International. Earth Quake ( 3 million) ... Very Limited microscopy and treatment at District level for the country's 90 ... – PowerPoint PPT presentation
Number of Views:1095
Avg rating:3.0/5.0
Title: Malaria in Pakistan
1
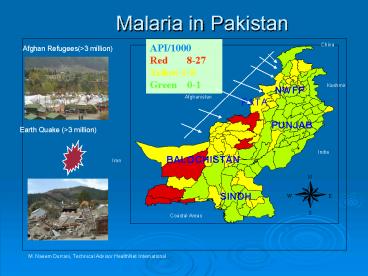
Malaria in Pakistan
API/1000 Red 8-27 Yellow 1-8 Green 0-1
China
Afghan Refugees(gt3 million)
Kashmir
Afghanistan
Earth Quake (gt3 million)
India
Iran
Coastal Areas
M. Naeem Durrani, Technical Advisor HealthNet
International
2
Malaria Control In Pakistan
- During the past two decades, the programme has
received very little attention and is considered
as a dying cadre at district and provincial level
in the Country. - Very Limited microscopy and treatment at District
level for the countrys 90 population at Risk.
(150 million) - Estimated 80 population seeks diagnosis and
treatment at under resourced and under skilled
Quasi private sector. - Focal IRS through countrys own limited resources
- Surveillance that need development
- Gaps Identified in 2003 for GF Round 2, project.
- Prioritized areas with high case load and prone
to epidemics - Strengthen and expand Microscopy.
- Build Capacities of Malaria related health
Personnel - Need for very heavy BCC component to bring
positive change in target populations behaviour
for timely utilization of malaria control
services. - Implementation of ITNs in 11 pilot districts/
tribal agencies.
3
Round 2 Project Objectives
- To ensure sustained functioning of 92 peripheral
microscopy centers 23 district, five provincial
and national malaria-training centre to improve
early diagnosis and prompt treatment at health
facility level including improving monitoring of
quality assurance standards at district level and
above. - To strengthen case management capacity of the
care providers and Monitoring Evaluation of the
project activities - To implement / continue a behavior change
communication (BCC) strategy to improve the
knowledge and decision making of general
population for access to diagnostic and or
treatment services within first 24 hours of onset
of fever and avail the benefits of simple and
safe preventive measures. - To introduce and promote the use of Long Lasting
Insecticide Treated Nets in selected districts
through public private partnership.
4
Implementing Partners
- Objective 1 Strengthening and Expansion of
Microscopy - DOMC
- Objective 2 Up gradation of technical and
management capacities of Malaria related health
personnel in 23 districts,
DOMC - Objective 3 BCC implementation, DOMC
- Objective 4 Implementation of ITNs in 11 pilot
districts - HealthNet, Green Star (PSI), NRSP
- DOMC SETS OVER AMBITIOUS TARGETS FOR ITSELF
5
Problems Encountered in Phase 1
- LFA did not assess the capacities of individual
SRs. - Lack of Clarity over GF system, policies and
procedures at all level (CCM,PR,SRs) A learning
phase for all - No continuity in Programme management, sharp
staff turn over of managers and technical staff - Serious delays in Procurements for both health
and non health items, ITNs were provided to SRs
in quarter 7 (18 months delay) - Serious delay in project staff recruitment at
DOMC. - Lack of Communication and Coordination between PR
and DoMC. - Public sector dominant CCM and its sub committees
failed to identify problems during course of
implementation, they learned about slow progress
when it was too late for remedial action. - Conflict of interests at various level in the
programme
6
Progress assessed by GF to decide on phase 2
Continuation
GF- HQ Decision after assessment based on
progress till Q-8 NO PHASE 2 EXTENSION
7
Way Forward.
- Consortium based Programs need to be reviewed
independently for each sub recipient every 2nd
quarter. - Greater role for INGOs/ bilateral Agencies to
develop public and private for profit sector to
deliver quality services. - Political commitment to ensure management
continuity through institutional reforms - Need for up-gradation of management Capacities at
program level. - Reform at CCM and its charter of mandate. Third
party PR, to avoid conflict of interest - An independent ME Committee with its own small
budget to assess progress regularly and keep CCM
informed on progress, problems and challenges. - Go for round 6 and subsequent rounds after the
IRM recommendations are available to add
credibility to the country proposal, Tasks should
be divided among SRs inline with their
capacities.
8
- THANK YOU