
Six Sensor CGM Array- Which do you trust? - PowerPoint PPT Presentation
1 / 14
Title:
Six Sensor CGM Array- Which do you trust?
Description:
... critical care Not suitable with abdominal diseases including peritonitis and abdominal surgery ... a. algorithm allowed us to avoid hypoglycemia ... – PowerPoint PPT presentation
Number of Views:101
Avg rating:3.0/5.0
Title: Six Sensor CGM Array- Which do you trust?
1
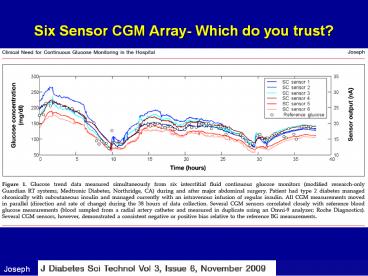
Six Sensor CGM Array- Which do you trust?
Data from subject D2
Joseph
2
Non-Closed Loop Insulin Administration Approaches
- A. Types- MD judgment, paper protocols,
order-entry systems, computerized algorithms - B. No adjustment for insulin sensitivity
(Portland, PID computer protocols)- - may take longer to goal
- C. Adjusts for Insulin Sensitivity- Yale, U.
Wash, Glucommander- faster but gt risk
hypoglycemia - Ideally, want BOTH faster, without
hypoglycemia - ULTIMATELY ALL SUFFER FROM HUMAN INTERFACE
ISSUES - SO COMPUTERIZED ALGORITHMS IN CLOSED-LOOP CGMS
DATA MAY BE SAFEST, LEAST RESOURCE INTENSIVE,
APPROACH - Ideally, adjustable goal - dial-in to fit
sensor issues, different ICUs, types of
patients, different ICU directors!
Steil,g., ICY insulin Delivery Algorithms, J.
Diabetes Sci Technol 3125,2009
3
Computerized Algorithms to Regulate Glucose in
ICU-Potential to Compensate for Imperfect Sensors
Patient safety Efficiency, nurse compliance
Decrease workload, reduce cognitive failure
Improve control, decrease hypoglycemia Proport
ional Integrative Derivative-
Proportional- absolute deviation, vs. goal,
Integral trends-
leads to basal insulin Derivative-
rate of change- leads to correction
factor Model Predictive Control- uses
multiple variables to model the
behavior of glu/ ins in
ICU- potential for less
variability- but if dont include an
important variable, can be off the track
Hoekstra Critical Care 2009,13223
4
Computerized Glucose Regulation in the ICU
PID advantage in hospital where multiple
variables May apply that are not in MPC model
!!! Or use MPC to monitor PID result, to
supervise/ detect possible sensor
failure/ Detect change in patient condition
5
Hospital Closed Loop discrete PID algorithm
From the Stanford PICU study. Data shows example
control achieved using reference blood glucose
(BG) readings and discrete PID insulin infusion.
Generation 4 sensor performance shown in blue
(2006 ADA).
6
Mathematical Modeling to predict glycemia in ICU
in order to Test Insulin Infusion Algorithms
eMPC
7
Methods- Sites of Delivery
- (1) multiple daily (subcutaneous) insulin
injection (MDII) - (2) continuous subcutaneous insulin infusion
(CSII) ,better - but not rapid enough effects for sudden changes
seen in critical care - (3) intravenous insulin infusion (IVII), best for
critical care - Drawbacks obstruction of insulin infusion
catheter, phlebitis, catheter related infection - (4) continuous intraperitoneal insulin infusion
(CIPII)- physiologic, but too many issues - Control is inferior to IVII in cases of high
BG variability, eg critical care - Not suitable with abdominal diseases including
peritonitis and abdominal surgery. - Catheter-related
complications (e.g., occlusions, aggregation of
insulin, local infections) - Production of anti-insulin antibodies.
- High cost
Meds to be delivered Glucose/ Insulin/
Glucagon- ? Incretin, Pramlintide
Hoshino, J Artif Organs (2009) 12141149
8
So, Given CGMS in ICU SETTING IS STILL HAMPERED
BY 1. Relative Inaccuracy of sensors 2. Site/
Sensor Issues 3. Changing Insulin Sensitivity
4. Human Interface Issues One can
have ALGORITHM ADJUST FOR THESE VARIABLES , but,
knowing error rates, ADJUST GOAL to AVOID
HYPOGLYCEMIA
9
Hyperinsulinemic-NormoglycemicClamp Technique in
Cardiac Surgery
70 non-DM 40 DM Target 3.5-6.1mM (This is a low
range, 65-110
Insulin 5mu/kg/min d20, varying
rates Hypoglycemia
lt60
Sato, Nutrition, 2010
10
Set algorithm 120mg (6.6 mM), to avoid
Hypoglycemiaeg Compensate for Imperfect
Sensors, Clinical variables-ePID, External
Closed-Loop Clinical Study
Aggregate Closed-Loop Results vs. Normal Glucose
Tolerant Profile (UCLA Clinical trial, n 10
T1DM, n 18 NGT)
Dial-up range one wishes!!
Diabetes 2006 55(12) 33443350.
11
JDRF Potential Pathway to an Artificial Pancreas
From Safety/ Regulary point of View
1
2
Very Low Glucose a Insulin Off Pump
Hypoglycemia Minimizer
START
END
12
How to Speed up?
13
Process- Where Do We Go From Here?Closed-
Loop Continuous Monitoring In Critical
Care--Back to the Future--
- SAFETY IS OVERRIDING PRINCIPLE- Aim for lowest
glucose possible without hypoglycemia (lt80 - Need Now- ROI exists-
- Live with what we have now- adjusting algorithms
to current sensor limitations- - Adjust DESIGN and USAGE of Imperfect Tools until
IDEAL available
Work Forward to Achieve Ideal
14
The Ultimate Goal Full Normalization of Glycemia
THANK YOU!!
Diabetes 2004 53(5) 12011207.
15
Self-Assessment Questionsmultiple choice
- 1. The most important aspect of Biostator use in
late 70s was - a. algorithm allowed us to avoid
hypoglycemia - b. blood testing vs. subcu was a major
advantage - c. easy, convenient to use
- 2. Current CGM Systems are imperfect tools to
avoid hypoglycemia in hospital now primarily
because - a. sensors inaccurate
- b. blood and subcutaneous tissue
measurements both suffer from time lag
issues - c. Use of information imperfectly applied
by humans in calculating insulin administration - 3. Closed-Loop CGMS can be used NOW as greatest
potential for achieving most benefit with least
risk to the patient (when govt permits)
because they can - a. eliminate vagaries of human dosing
- b. algorithms can be calculated to adjust
for inaccuracies of measurement - c. algorithms/ technology actually
exist that achieve this (since 1979) - d. all of above
Recommended
CrystalGraphics Presentations





























