
Present Study - PowerPoint PPT Presentation
Title:
Present Study
Description:
Resulted in piece wise motion of modeled CoP Non-smooth GRF ... Prediction pathologic gait 3-D kinematics collected via Vicon implementing a 38 marker Helen-Hayes ... – PowerPoint PPT presentation
Number of Views:68
Avg rating:3.0/5.0
Title: Present Study
1
Patient Specific Motion Modeling and Assistive
Devices
S Russell, P Sheth, B Bennett, P Allaire, M Abel
University of Virginia, Motion Analysis and Motor
Performance Laboratory, Charlottesville, VA.
INTRODUCTION
RESULTS (cont)
METHODS (cont)
Angular Momentum Control
- Foot Model
- Previous model consisted of
- only heel and toe ellipsoids
- Resulted in piece wise motion
- of modeled CoP
- Non-smooth GRF
- New model includes contact
- ellipsoids along metatarsals
- connecting heel/toe ellipsoids
- Smooth/continuous GRF
- Facilitates smooth CoP motion in
- both sagittal and frontal planes
- Angular Momentum used to develop stable walking
in bipedal gait models (Goswami, Popovic) - Previously used to
- Determine energy lost at heel strike/foot contact
- Control strategy for full body model in single
support
Present Study
- Develop patient specific full body gait model
- Develop applied joint torques from desired
Angular Momentum - Implementation of newly developed foot model
- Application and validation of Optimized contact
model between foot and floor
Angular Momentum Control
- Angular momentum of each segment about the body
CoM calculated and averaged for each test subject - Data used to populate 19xN matrix A where
- N data points over gait cycle
- PD control used to determine joint torques for
each point of gait cycle, 1,2,N - Simulations run using angular momentum A as
negative feedback for PD control resulting in
minimized error between desired and simulated
angular momentum
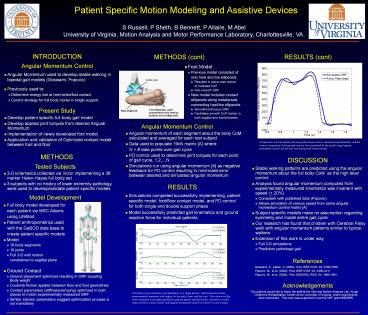
Comparison of actual patient vertical ground
reaction force, measured experimentally, and the
vertical component of the ground reaction force
predicted by the model using Angular momentum
control and the new foot and ground contact model.
METHODS
DISCUSSION
Tested Subjects
- Stable walking patterns are predicted using the
angular momentum about the full body CoM as the
high level control - Analysis found angular momentum computed from
experimentally measured kinematics was invariant
with speed ( 20) - Consistent with published data (Popovic)
- Allows simulation of various speed from same
angular momentum control matrix A - Subject specific models make no assumption
regarding symmetry and model entire gait cycle - Our research has found that children with
Cerebral Palsy walk with angular momentum
patterns similar to typical walkers - Extension of this work is under way
- Full 3-D simulations
- Prediction pathologic gait
- 3-D kinematics collected via Vicon implementing a
38 marker Helen-Hayes full body set - 3 subjects with no history of lower extremity
pathology were used to develop/validate patient
specific models
RESULTS
- Simulations completed successfully implementing,
patient specific model, foot/floor contact model,
and PD control for both single and double support
phase - Model successfully predicted gait kinematics and
ground reaction force for individual patients
Model Development
- Full body model developed for
- each patient via MSC.Adams
- using LifeMod
- Patient anthropometrics used
- with the GeBOD data base to
- create patient specific models
- Model
- 19 body segments
- 16 joints
- Full 3-D with motion
- constrained to sagittal plane
- Ground Contact
- Ground placement optimized resulting in GRF
equaling Body weight - Coulomb friction applied between floor and foot
geometries - Contact parameters (stiffness/damping) optimized
in both planes to match experimentally measured
GRF - Similar solution parameters suggest optimization
process is not mandatory
References
Goswami, A., Kallen, V. (2004). Proc IEEE ICRA
04, 3785-3790. Popovic, M., et al. (2004). Proc
IEEE ICRA 04, 2405-2411. Popovic, M., et al.
(2004). Proc IEEE/RSJ IROS 04, 1685-1691.
Acknowledgements
The authors would like to thank the staff at the
Gait and Motion Analysis Lab, Kluge Childrens
Rehabilitation Center at the University of
Virginia, where experiments were conducted. This
work was supported in part by NSF grant 0503256.
Plots show lower extremity joint kinematics of a
single patient. Results shown include
experimentally measured joint angles for the
ankle, knee, and hip joint. Also shown are the
lower extremity joint angles predicted using the
patient specific model, revised foot model,
improved floor contact model, and angular
momentum based PD control for joint torques
2
Patient Specific Motion Modeling and Assistive
Devices
S Russell, P Sheth, B Bennett, P Allaire, M Abel
University of Virginia, Motion Analysis and Motor
Performance Laboratory, Charlottesville, VA.
INTRODUCTION
Present Studies
Cerebral Palsy
- Develop plantar flexion assist ankle foot
orthosis (AFO) to promote heel strike while
facilitating 3 rockers of stance - Develop passive brace to store energy lost at
heel strike and return it during pre swing - Develop motorized walker to predict gait events
and assist subjects in walking and turning
- 764,000 people in the United States have symptoms
of Cerebral Palsy (CP) - Metabolic costs of walking 2-3 times higher in
individuals with CP - 50 of people with CP are prescribed Ankle Foot
Orthotics (AFO) - Previous research equivocal on effectiveness of
AFOs
Smart Walker
Energy Return AFO
Plantar Flexion Assist AFO
Objectives
Objectives
Objectives
- Develop an AFO which limits plantar flexion
during swing due to conditions such as equinus or
drop foot - Allow patient kinematics to exploit all three
rockers during stance (Figure 1)
- Energy added from ankle plantar flexion at push
off for CP gait typically 15-20 less than normal
gait - Develop an AFO to store the energy lost during
heel strike and return the energy later in gait
cycle (i.e. push off) - Return .4 J/kg of energy to gait at push off (15
total normal energy added at push off) - Allow patient kinematics to exploit all three
rockers during stance (Figure 1)
- Preform real-time prediction of gait events (i.e.
heel strike, toe off) via forces applied to
walker handles - Create shared control of a motorized posterior
walker to facilitate better walking in children
with CP
Previous Solutions
Figure 1. 1st Rocker represents rotation about
the heel at initial heel contact allowing the
foot to lay flat, 2nd Rocker allows the body to
progress forward rotating about the ankle with
the foot flat in stance, and the 3rd rocker
allows the subject to rotate onto the ball of
there foot to facilitate push off during pre
swing.
- Post-processing prediction of gait events from
handle forces validated using VICON motion
analysis - Implementation of shared control on steering
angle to control anterior walker trajectories
Current AFOs
- Solid ankle AFOs are unable to return energy to
gait cycle while PLS, ground reaction, and carbon
toe off AFOs store and return energy at push off
but do so by inhibiting the 2nd rocker
Current AFOs
- Solid ankle AFOs and posterior leaf spring (PLS)
restrict or inhibit one or more kinematic rockers - Hinged AFOs facilitate rockers but cannot
inhibit foot drop or equinus
Current Solution Design
Current Solution Design
- Based on a double upright AFO with dual action
joints - Patient specific conical compression springs
located between foot bed and sole of shoe - Ankle plantar flexion compresses the springs via
the cable, moment arm, and pulleys - Spring tension is adjusted to apply patient
specific plantar flexion assist during swing
phase - In stance springs are compressed as weight is
transferred forward releasing tension on moment
arm facilitating full range of motion and all 3
rockers
- Development of real time prediction of Gait
events from forces applied to walker handles
during walking - Development of shared control algorithm to
control electric motors for desired walker motion - Hold walker position fixed in cases of impending
fall (instability) - Interject energy during strategic gait events
(push off) - Facilitate directional control of walker
- Negate additional work of dragging a walker
during gait
- An additional benefit of the design is the energy
return applied during pre swing to aid push off
as the springs decompress as body weight is
removed
Current Solution Design
- Energy stored at heel strike
- Body weight compresses springs
- Springs held in compression by multi-tooth
ratchet system - Tension in cables released to facilitate full
range of motion - Energy returned during push off
- Body rotates forward over foot (2nd rocker)
- Foot is dorsi-flexed taking slack out of cable
- Weight in on ball of foot activating mechanism to
release springs - Springs create plantar flexion moment about ankle
joint via cables
Recommended
CrystalGraphics Presentations





























