
Lumbar Puncture - PowerPoint PPT Presentation
Title:
Lumbar Puncture
Description:
Lumbar Puncture Interpretation Low CSF Glucose Syndromes Bacterial meningitis Syphilis Tuberculous meningitis Chemical meningitis Fungal meningitis Subarachnoid ... – PowerPoint PPT presentation
Number of Views:211
Avg rating:3.0/5.0
Title: Lumbar Puncture
1
Lumbar Puncture
2
objectives
- To know the indication and contraindication for
lumber puncture. - To know the technique of insertion of the lumber
puncture. - Too know the complication of lumber puncture.
3
CSF Formation
- 140 ml spinal and cranial CSF
- 30 ml in the spinal cord
- Production is approx. 0.35 ml/min
- Net flow out of ventricles 50 100 ml/day
- Reduces brain weight from 1400 to 50g.
4
Indications for Lumbar Puncture
- 1- diagnosis of CNS infection
- 2-suspection of spontaneous subarachnoid
hemorrhage - 3- evaluation and diagnosis of demyelinating or
inflammatory CNS process .
5
- 4- infusion of anathesia,chemotherapy,or contrast
dye into spinal canal - 5- treatment of idiopathic intracranial
hypertension
6
Infectious Indications
- Fever of unknown origin
- Children 1mo to 3yrs fever, irritability, and
vomiting. Cannot comfort child - Over age 3yrs nuchal rigidity, Kernigs sign,
and Brudzinskis sign - Petechial rash in a febrile child
- Partially treated children are less likely to be
febrile or exhibit an altered mental status
7
Subarachnoid Hemorrhage
- Diagnosis usually made by CT scan or by blood in
CSF. - Initial presentation CT 92-98 accurate
- Later than 24 hr presentation 76 accurate
- After initial leak, CT is usually negative
8
Contraindications for LP
- 1-Absolutely contraindicated in the presence of
infection in the tissues near the puncture site. - 2-suspesion of increase intracranial pressure
due to cerebral mass. - Caution advised when lateralizing signs or signs
of uncal herniation.
9
- 3- uncorrected coagulopathy
- 4-acute spinal cord trauma
10
- Technique of insertion
11
Equipment
- Spinal needle
- Less than 1 yr 1.5in
- 1yr to middle childhood 2.5in
- Older children and adults 3.5in
- Three-way stopcock
- Manometer
- 4 specimen tubes
- Local anesthesia
- Drapes
- Betadine
12
Procedure
- Almost all patients are afraid of an LP.
Explaining the procedure in advance and
discussing each step aids in reducing anxiety. - Inquire about allergies to anesthetics.
- Informed consent.
13
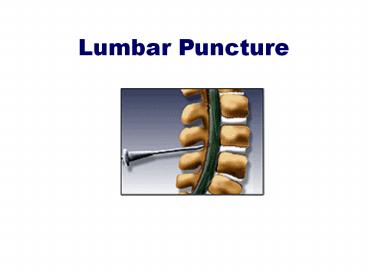
positioning
- Performed with the patient in the lateral
recumbent position. Or sitting upright - A line connecting the posterior superior iliac
crest will intersect the midline at approx. the
L4 spinous process. - Spinal needles entering the subarachnoid space at
this point are well below the termination of the
spinal cord.
14
(No Transcript)
15
Site of injection
- In the adult, the spinal cord extends to the
lower level of L1 or the body of L2. - LP in adults and in older children may be
performed from L2 to L3 interspace to the L5 to
S1 interspace. - At birth, the cord ends at the level of L3.
- LP in infant may be performed at the L4 to L5 or
L5 to S1 interspace.
16
(No Transcript)
17
steps
- Position the patient
- Generally performed in the lateral decubitus
position. - A pillow is placed under the head to keep it in
the same plane as the spine. - Shoulders and hips are positioned. perpendicular
with the table. - Lower back should be arched toward practitioner.
18
Insertion
- Sterile gloves MUST be used.
- Wash back with antiseptic solution.
- Sterile towel under hips.
- The skin and deeper subcutaneous tissue are
infiltrated with local anesthetic. - Warn patient of transient discomfort of
anesthetic.
19
- 6-Anesthetizing the deeper subcutaneous tissue
significantly reduces the procedure discomfort. - -Some operators not only anesthetize the
interspinous ligament but also apply local
anesthesia in a vertical fanning distribution on
both sides of the spinous processes near the
lamina.
20
- 7-The patient should be told to report any pain
and should be informed that he or she will feel
some pressure. - 8-The needle is placed into the skin in the
midline parallel to the bed. - 9-The needle is held with both thumbs and index
fingers.
21
- 10-After the subcutaneous tissue has been
penetrated, the needle is angled toward the
umbilicus. - 11-The bevel of the needle should be facing
laterally (toward patients side).
22
- The ligaments offer resistance to the needle, and
a pop is often felt as they are penetrated. - Clear fluid will flow from the needle when the
subarachnoid space has been penetrated.
23
- 11-If bone is encountered, withdrawal into
subcutaneous tissue and redirect. - 12-Attach a manometer and record opening
pressure. - 13-Turn stopcock and collect fluid.
- Withdrawal needle and place a dressing.
24
- Tube 1 is used for determining protein and
glucose - Tube 2 is used for microbiologic and cytologic
studies - Tube 3 is for cell counts and serologic tests for
syphilis
25
(No Transcript)
26
- Ligament flavum is a strong, elastic, yellow
membrane covering the interlaminar space between
the vertebrae. - Interspinal ligaments join the inferior and
superior borders of adjacent spinous processes. - Supraspinal ligament connects the spinous
processes
27
(No Transcript)
28
Interpretations
- Pressure
- Opening pressure is taken promptly, avoiding
falsely low values due to leakage through and
around the needle - Normal pressure is between 70 and 180 mm H20
29
Interpretation
- Appearance
- If CSF is not crystal clear, a pathologic
condition of the CNS should be suspected - Compare fluid to water
- Fluid may be clear with as many as 400 RBCs/mm3
and 200 WBCs/mm3
30
Interpretation
- Cells
- WBC counts over 5 cells/mm3 should be taken to
indicate the presence of pathologic condition - Polymorphonuclear leukocytes are never seen in
normal adults - Neutrophilic pleocytosis is commonly associated
with bacterial infections or early stages of
viral infections, tuberculosis, meningitis,
hematogenous meningitis, and chemical meningitis
due to foreign bodies.
31
Interpretation
- Cells
- Eosinophils are always abnormal and most commonly
represent a parasite infestation. - Eosinophils have also been reported in cases of
subarachnoid hemorrhage, lymphoma, Hodgkins
disease, brucellosis, fungal meningitis,
mycoplasma pneumonia infection, measles,
lymphocytic choriomeningitis, rickettsial
infections, leukemia, demyelinating disease,
sarcoiodosis, acute inflammatory demyelinating
polyneuropathy, allergic reactions, and
idiopathic eosinophilic meningitis.
32
Interpretation
- Cells
- Normal CSF RBCs are less than 10/mm3.
- Counts that are otherwise unexplained may be due
to a traumatic tap. - Herpes simplex virus encephalitis may elevate the
CSF RBC count in many patients.
33
Interpretation
- Glucose
- Low CSF glucose concentration indicates increased
glucose use in the brain and the spinal cord. - The normal range of CSF glucose is between 50 and
80 mg/dl - 60-70 of serum glucose concentration
- Only low concentrations of glucose are
significance
34
Interpretation
- Low CSF Glucose Syndromes
Bacterial meningitis Syphilis
Tuberculous meningitis Chemical meningitis
Fungal meningitis Subarachnoid meningitis
Sarcoidosis Mumps meningitis
Meningeal carcinomatosis Herpes simplex encephalitis
Amebic meningitis Hypoglycemia
Cysticercosis Trichinosis
35
Interpretation
- Protein
- Increase in CSF total protein levels are a
nonspecific abnormality associated with many
disease states. - Levels gt 500mg/dl are uncommon and are seen
mainly in meningitis, in subarachnoid bleeding,
and with spinal tumors.
36
The Traumatic Tap
- It should not be difficult to distinguish between
subarachnoid hemorrhage and a traumatic tap. - In traumatic taps, the fluid generally clears
between 1st and 3rd tubes.
37
CSF Analysis with Infections
- Bacterial Infections
- The Gram stain is of great importance, because
this often dictates the initial choice of
antibiotic. - Gram-negative intracellular or extracellular
diplococci are indicative of Neisseria
meningitidis - Small Gram-negative bacilli may include
Haemophilus influenza, especially in children. - Gram-positive cocci indicates Streptococcus
pneumoniae, other Streptococcus species, or
Staphylococcus. - 20 of Gram stains may be falsely negative.
38
CSF Analysis with Infections
- Bacterial Infections
- While the culture is pending, one may suspect a
bacterial infection in the presence of an
elevated opening pressure and a marked
pleocytosis ranging between 500 and 20,000
WBCs/mm3. - The differential count is usually chiefly
neutrophils. - A count above 1000 cells/mm3 seldom occurs in
viral infections.
39
CSF Analysis with Infections
- Bacterial Infections
- CSF glucose levels less than 40 mg/dl or less
than 50 of a simultaneous blood glucose level
should raise the question of bacterial
meningitis. - The CSF protein content in bacterial meningitis
ranges from 500 to 1500 mg/dl.
40
CSF Analysis with Infections
- Viral Studies
- The organisms most commonly isolated in viral
meningitis are enteroviruses and mumps. - Enteroviruses summer and fall
- Mumps winter and spring
41
CSF Analysis with Infections
- Viral Studies
- WBC count in viral meningitis and encephalitis
usually 10 to 1000 cells/mm3. - The differential count is predominantly
lymphocytic and mononuclear in type. - Protein levels are usually mildly elevated
- Antibiotic coverage pending culture results may
be reasonably initiated pending culture results
if in doubt.
42
Complications
- Headache After Lumbar Puncture
- Most common complication
- Occurs 5-30 of all spinal taps
- Usually starts up to 48 hours after to procedure.
- Usually lasts 1-2 days (occas 14 days)
43
Complications
- Headache After Lumbar Puncture
- Usually begins within minutes after arising and
resolves with recumbent position. - Pain is mild to incapacitating and is usually
cervical and sub-occipital, but may involve the
shoulders and the entire cranium.
44
Etiology of headache after LP
- 1- leakage of fluid through dural puncture site.
- 2- low CSF pressure.
- 3- some contributing factors as
- The diameter of the needel,the shape of the
needel,the use of spinal anesthesia
45
How to minimize the headache?
- 1-choice of needle standerd Quinck versus
atraumatic . - 2- decrease the number of attempts
- 3-reinsersion of the stylet
- 4- bed rest after the proceedures
46
- Headache After Lumbar Puncture
- Incidence is higher in younger patients and
females, and those with headache history. - Treatment barbiturates, fluids, caffeine (500mg
in 2 ml NS IV push) more common 500mg in 2 L over
1 hr.
47
- Thank you