
Exam of the Abdomen - PowerPoint PPT Presentation
1 / 93
Title:
Exam of the Abdomen
Description:
1 Exam of the Abdomen The importance of abdominal examination The importance of abdominal examination Measurement of liver Etiology of hepatomegaly ... – PowerPoint PPT presentation
Number of Views:136
Avg rating:3.0/5.0
Title: Exam of the Abdomen
1
????1
Exam of the Abdomen
2
The importance of abdominal examination
3
The specialities of abdominal examination
1?Perform in order inspection,auscultation,percus
sion ,palpation Record in order
inspection, palpation, percussion,
auscultation 2?Palpation is of the highest
importance 3?Perform gently 4?Pay attention to
patients expression 5?There are superficial
palpation, deep palpation et al?
4
Study method
How to perform all the itemsabnormal
findingsclinical meaning
Longitudinalcomprehensive I, A,P,Pa thinking
the whole body idea Transverse
differential diagnosisspecial point thinking
different itemsthe same purpose
e.g. Shifting
dullness
fluid wave
ascites
puddle test
5
Surface markings and regions of abdomen
(anatomy basis)
1?costal margin 2?xiphoid process 3?upper
abdominal angle 4?umbilicus 5?anterior superior
iliac spine 6?lateral border of reclus muscles
(gallbladder point) 7?midabdominal
line 8?inguinal ligament 9?costo-vertebral angle
6
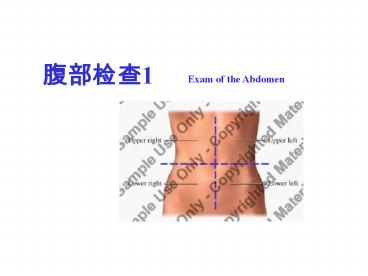
- A surface map of the abdomen
- used to describe the location of
- abnormalities
- two systems of mapping
7
Four quadrants of the abdomen
8
Nine quadrants of the abdomen
Epigastric region
Right hypochondrial region
Umbilical region
Right lumbar region
Right iliac region
Hypogastric region
9
Strong point weak point
10
Abdomen anatomy
11
Abdomen anatomy
12
(No Transcript)
13
Sigmoid colon Left ovary
14
Descending colon Small bowel Left kidney
15
Spleen Colon stomach
16
Stomach Duodenum Tr colon Aorta Pancreas liver
17
Liver Gallbladder Duodenum
18
Ascending colon Right kidney
19
Appendix Caecum Right Ovary Small bowel
20
Bladder Uterus Small bowel
21
Patients Position supine position
enough exposure comfortable relaxed
raise his head and shoulders a few inches
and slightly flex his knees and hips.
Approach from the right side
22
Abdominal examination
Inspection
contentsappearance(normal appearance)
skin (superficial) veins
breath movement
gastric or intestinal pattern and
peristalsis inguinal area
hernia umbilicus
throbbing in the epigastric
region
23
Inspection
Abdominal appearance
Global abdominal enlargement(distension)
fluid ascites(abdominal circumference)
air in the stomach or intestine,
pneumoperitoneum
fat obesity abdominal mass in
large size differentiate obesity
from ascites(frog belly) apical
belly
Local enlargementinside or outside
position contour breath motility throbbing
valsava Global abdominal concauityscaphoid
abdomen
24
Global abdominal enlargement
25
(A) obesity or gaseous distension the umbilicus
is inverted. (B) ascites the umbilicus is
everted. (C) The scaphoid (boat-shaped)
configuration of slender people. (D) a lower
abdominal mass, a distended bladder for example.
(E) an upper abdominal mass, an enlarged liver,
for example
26
Inspection
Skin
skin eruptionherpes zoster Pigmentation and
color Cullen Sign, Grey-turner Sign
Spider Angiomata stria(e) scar hair
27
Spider Angiomata - dilated arterioles, most often
visible on the skin of the upper chest
Liver cirrhosis
28
massive retroperitoneal bleeding (classically in
severe acute pancreatitis) the blood dissects
around the flanks between the fascial layers
below the subcutaneous fat to reach the
subepidermal tissue on the anterior abdomen,
either in the flanks (Grey-turner Sign) or about
the umbilicus (Cullen Sign).
29
Abdominal striae the rupture of
subepidermal connective tissue
abdominal distension reddish or pink
fades to white large doses of
corticosteroids remain pink until the
dosage is reduced.
30
Inspection
Abdominal superficial veins
How to determine the direction of blood flow
???
Portal hypertension Budd-Chiari syndrome
31
?????????
32
Breath movement
Decrease or disappearance peritonitis,
ascites
gastric or intestinal pattern and
peristalsis Obstruction
33
Inspection
hernia umbilicus
inguinal area throbbing in the
epigastric region
34
throbbing in the epigastric region
Right ventricle Increase with deep breath
Aorta Decrease with deep
breath
The most common cause of a pulsative liver
tricuspid incompetence.
35
36
37
Caput medusae
38
(No Transcript)
39
Auscultation
bowel sounds Bruits(murmur)position?
time(murmurs of artery or vein) friction
rubs scratch test(????) puddle test(????)
40
Bowel Sounds
Are bowel sounds present? If present, are
they frequent or sparse (i.e.quantity)?
What is the nature of the sounds (i.e. quality)?
Hyperactiveintestinal infection, hemorrhage,
laxative
High-pitchedmechanical ileus
(loud bowel sounds accompany cramping
abdominal pain or abdominal
distension) Hypoactiveperitonitis?hypokalemia?hy
pomotility The absence of bowel sounds
peritonitis
41
(No Transcript)
42
--------friction rub, a rare finding,
The viscera near the diaphragm move with
respiration and rub peritoneal surfaces together.
When there is peritonitis in the upper abdomen
without much exudate, the rubbing of the inflamed
peritoneal surfaces produces a dry, soft,
scraping sound
heard early in the course of peritonitis.
occurs in splenic infarction,
in neoplastic disease that involves
the surface of the liver, in
abscess formation in either organ.
43
Puddle test
Have the patient lie prone for 5 minutes and then
have him rise to his elbows and knees. Put your
stethoscope to lowest point of the midline and
begin tapping or flicking with a consistent force
in the patient's flank on the side toward you.
You move your stethoscope diaphragm away from the
midline to the far side of the abdomen while you
flick constantly in the same place. When the
diaphragm of the stethoscope reaches the far side
of a puddle of ascitic fluid, the sound produced
by the flicking changes.
44
Percussion
RMCL(5C.M,9-11cm) RMAL(7-10) R scapular line(10)
????? relative Liver span(figure) absolute
enlarge reduce,
disappear,?????
Reduce acute necrotic hepatitis
liver cirrhosis( often late stage)
Disappear gastrointestinal perforation
(emergency)
45
(No Transcript)
46
????? pain elicited by percussion over liver
hepatitis,
liver abscess, hemotoma
47
(No Transcript)
48
Percussion
Traube area
Margin, location, size, clinical meaning of
decrease or disappearance
49
Percussion
Spleenmidaxillary line,9-11,4-7cm,
not surpass anterior axillary line
shifting dullness
Differentiate with ascites
fluid inside intestine huge
ovary cyst
50
(No Transcript)
51
Percussion
Percussion of bladder costo-vertebral angle
tenderness (CVAT) pounding gently with the
bottom of your fist on the costo-vertebral
angle will cause pain if the underlying
kidney is inflamed.
(
)
52
Percuss costo-vertebral angle
53
Etiology of costo-vertebral angle percussion pain
Often bilateral sides glomerulonephritis
interstitial nephritis
Often one side nephrolithiasis( kidney stone)
pyelopephritis
Tuberculosis
54
Thank you!
55
????2
Exam of the Abdomen
56
Seven quadrants
57
Palpation
position Methodssuperficial?deep Performance
ordercounter-clockwise begin by asking
if there is pain at some area and
proceed accordingly. Cooperation with
breath Patient as relaxed as possible
58
Palpation
Tips
Warm your hand and stethoscope Talk with the
patient to make him relaxed Cooperate with
breath Use the patients hand if he is very
sensitive.
59
Superficial palpation
60
Deep palpation
61
Hooking edge of the liver
62
Palpation
Tense of abdominal wallboard-like rigidity,
dough kneading
sensation tendernessposition(AMI, Pneumonia,
pleurisy) rebound tenderness
peritoneal irritation sigh pain
with cough,breath,percussion
Mc Burney point
63
Palpation
Organsliver?spleen?kidneys?
gallbladder?bladder?pancreas
Solid organs
Size, texture, margin, surface, Tenderness,
throbbing, friction
64
Palpation
Livermaneuver sizecostal
margin(2cm),xiphoid process(3cm)
texturelip soft, nose moderately hard,
forehead hard margin and surface
tenderness
throbbing?friction hepatojugulor
reflex ?-?????
65
(No Transcript)
66
Measurement of liver
67
Etiology of hepatomegaly
Hepatitis neoplasm (localized) fatty liver -
secondary to diabetes, toxins haematological
disease chronic myeloid leukemia
lymphoma right heart failure Liver
abscess (localized) extra-hepatic biliary tract
obstruction
68
Palpation
Spleen position measurement of
splenomegaly degree of splenomegaly
Characteristics
Movement to RLD with inspiration A notch may be
palpable The dullness on percussion extends above
costal margin
69
Differentiate from
Enlargement of left lobe of liver Enlargement of
Left kidney Splenic flexure of colon Cyst of
pancreatic tail
Dullness to percussion A notch
70
(No Transcript)
71
Mild
2cm
Severe
72
(No Transcript)
73
Etiology of splenomegaly
- Signs of chronic liver disease
- Generalized lymphadenopathy
- Size of spleen
74
Etiology of splenomegaly
- Signs of chronic liver disease
- Portal hypertension(liver
cirrhosis) - Generalized lymphadenopathy
- lymphoproliferative
disease(lymphoma) - Size of spleen
- severe chronic myeloid leukemia
- myelofrosis
- kala-azar
75
Etiology of splenomegaly
Common causes
Portal hypertension liver cirrhosis,
Budd-Chiari syndrome lymphoproliferative
disease lymphoma leukemia Infection
sub-acute bacterial endocarditis
76
GallbladderMurphys sign
Courvoisiers sign
kidney
Up and lower points of Ureter Costo-vertebral
point Costo-lumbar point
77
(No Transcript)
78
(No Transcript)
79
Kidney palpation
80
Palpation
Mass
palpable Tendinous inscription of rectus
abdominis Tr. Colon, sigmoid
colon,cecum, lumbar vertebrates and
sacropromontory
massposition, size, contour, soft or hard,
tenderness motility,throbbing
inside or outside abdominal cavity
81
(Sigmoid colon)
82
Palpation
??? succusion splash ???? fluid wave
83
succusion splash
A large volume of fluid and air may collect in
the stomach. You can shake the abdomen and hear
the splash at the fluid-gas interface, often
without a stethoscope. You can hear this easily
in a normal person who has recently eaten or
drunk a reasonable volume It occurs long after
meals in cases of gastric outlet obstruction.
84
Assessing for a fluid wave
85
Special maneuver
Iliopsoas test ????? Obturator maneuver
?????? Referred tenderness ????? Rovsing test
?????? Palpation of aorta
86
Abnormal findings of liver cirrhosis
Hyperbilirubinemia The diseased liver may be
unable to conjugate or secrete bilirubin
appropriately. This can lead to Icterus - Yellow
discoloration of the sclera. Jaundice - Yellow
discoloration of the skin. Bilirubinuria -
Golden-brown coloration of the urine.
87
Abnormal findings of liver cirrhosis
Ascites Increased Systemic Estrogen Levels
Breast development (gynecomastia).
Spider Angiomata Lower Extremity
Edema Impaired synthesis of the protein albumin
leads to lower intravascular oncotic pressure and
resultant leakage of fluid into soft tissues.
This is particularly evident in the lower
extremities. Varices Caput Medusae Spelnomegaly
88
Abdominal exam of liver cirrhosis with ascites
Inspection
Jaundice Spider agiomata Umbilical hernia global
enlargement Varices Caput Medusae Decrease of
abdominal breath
Auscultation
Venous hums- Caput Medusae
89
Abdominal exam of liver cirrhosis with ascites
Percussion
Shifting dullness splenomegaly
Palpation
Splenomegaly Fluid wave
90
(No Transcript)
91
(No Transcript)
92
gynecomastia
93
(No Transcript)
Recommended
CrystalGraphics Presentations





























