
Loss and Grief for Children and Adolescents - PowerPoint PPT Presentation
1 / 30
Title:
Loss and Grief for Children and Adolescents
Description:
... Canterbury 1970-74 Child Psychotherapy (Ken Munro Fraser) Structural Family Therapy ... Gestalt therapy Group therapy Strategic Family ... Family Therapy ... – PowerPoint PPT presentation
Number of Views:1451
Avg rating:3.0/5.0
Title: Loss and Grief for Children and Adolescents
1
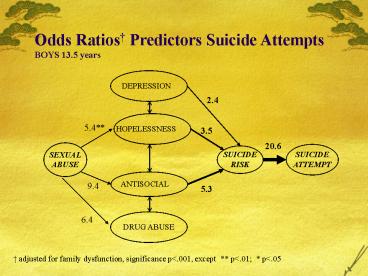
Odds Ratios Predictors Suicide Attempts BOYS
13.5 years
2.4
5.4
3.5
20.6
9.4
5.3
6.4
adjusted for family dysfunction, significance
plt.001, except plt.01 plt.05
2
The changing face of mental health services
3
In the 80s
- We dealt more with
- Anxiety Disorders
- Depression
- Developmental problems
- Minor behavioural problems
- Drug induced psychosis and ADHD were rare
- Bipolar Disorder Aspergers almost unknown
4
In the new Millennium
- Serious conduct disorder and delinquency (for
which we have a limited skill set) - Self-harming behaviours (60 of our CYMHS
referrals in a recent survey) - Drug induced psychosis (where we are fighting a
losing battle) - A wide range of disorders which may have their
origins in Poor Attachment and Social Exclusion
(where social change is necessary, which may be
outside our ambit)
5
In the new Millennium
- Family Crises (more families seem unable to cope
with normal developmental transitions) - Depression (which may itself have origins in Poor
Attachment and Social Exclusion) seems to be at
epidemic proportions, and is overwhelming our
skill set, but. - Anxiety Disorders (for which we have a rich skill
set) are now the hidden calamity (particularly
Social Phobia)
6
(No Transcript)
7
Antidepressant Use 1995 (Number)
MALE FEMALE
0-14 15-24 0-14 15-24
Amitryptiline 1727
Dothiepin 2198 724
Doxepin 199 41 178
Fluoxetine 852 63 2134
Other 27,292 4083 4940 2845
Total 27,491 7,134 5044 7417
ABS, 1999
8
Medication Use (18-34 yrs)NHS Survey 2005
- 704,200 used psychotropics
- 41,548 (5.9) Citalopram
- 25,351 (3.6) Paroxetine
- 51,407 (7.3) Sertraline
- 11,972 (1.7) Other SSRI
- 20,422 (2.9) Venlafaxine
- 12,676 (1.8) Tricyclics
- 12,676 (1.8) Other Antidepressant
- 10.1 Anxiolytics
- 83.5 other including 69.2 Vitamins and Minerals
- Table 15, page 36 Ausstats 2005
18.5 Total SSRIs
9
Western Australian Child Health Survey Children
with Mental Health Problems
Number (000) Per cent Males 30.0 20.0 Fe
males 23.5 15.4 4 to 11 year
olds 30.8 16.0 12 to 16 year
olds 22.7 20.6 All children 53.5 17.7
as determined by caregiver and teacher using
the Child Behavioural Checklist
Zubrick et al 1995
10
Mental Behavioural Problems, 2005
0-14 Rate 15-24 Rate
Alcohol/Drug np 19,000 0.71
Mood Disorders 30,300 0.77 144,600 5.4
Anxiety 89,700 2.3 123,600 4.6
Psychol Devel 100,600 2.57 60,800 2.26
Behavioural 116,300 2.97 34,700 1.29
Other 19,400 0.49 21,000 0.78
Symptoms/Signs 8,300 0.21 7,600 0.28
Total 263,000 6.71 267,800 9.94
Population Total 3,920,600 2,693,000
11
My own experience
12
A PERSONAL CONTEXT
- London 1968-9
- Analytic psychotherapy (Irving Kreeger, Gordon
Stuart Prince) - Hypnosis (Marcuse)
- Behaviour Therapy (Marks and Gelder)
- Canterbury 1970-74
- Child Psychotherapy (Ken Munro Fraser)
- Structural Family Therapy (Minuchin)
- 25 bed inpatient Unit
13
A PERSONAL CONTEXT
- Adelaide 1974-82 (Childrens Hospital)
- Infant Observation
- Child and Adolescent Psychotherapy
- Transactional Analysis (Berne)
- Gestalt therapy
- Group therapy
- Strategic Family Therapy (Gerard, Epstein, Haley)
- Systemic Family Therapy (Palazzoli et al)
- Narrative Therapy (White, Epston)
14
A PERSONAL CONTEXT
- Private Practice 1982-86
- Expert Family Therapy group 2 years
- Flinders Medical Centre 1986-2001
- Cognitive Behavioural Therapy
- Individual Therapy
- Family Therapy (Screens and Teams)
- Solution Focussed Therapy (de Shazer and Insoo
Kim Berg 1990)
15
A Note about Private Practice
- Solid Clinical Work
- 10-12 hours per day, on the hour every hour
- 600 new cases in 4 years - ie about 3 new cases
per week - Some school visits
- Some supervision and Teaching of registrars
- Art classes one afternoon a week to preserve
sanity
16
If you want effectiveness and efficiency in a
service, there is no substitute for highly
skilled, well supervised, experienced clinicians.
17
Clinical Work
- Central to what we do
- Yet we can never be quite certain what goes on in
the consulting room - No measures, no online reporting, no audio can
really tell you what goes on - Current administrative attempts to find out are
self serving and overwhelm the clinical process - The best Risk Management is to have good
clinicians
18
On Entry to Clinical Service
- 2 week full time Orientation Program
- 16 week twice a week therapy training program in
house - Option for lengthy training and supervision with
expert therapists (eg Malcolm Robinson or Michael
White for CAMHS in South Australia) with service
sharing the cost and the time cost.
19
Clear Clinical Expectations
- 1-2 new cases a week
- ie 70-75 per annum on average (range 50-100)
- For 30 therapists in a service you could manage
about 2200 new cases - 10 clinical follow-ups a week
- ie about 500 follow-up per annum
- For 30 therapists about 15,000 slots per annum
20
Therapist Burnout
- Too little training
- Too little supervision
- Too little variety
- Too many cases
- Too much paperwork
- Important to provide enrichment - special project
development, teaching, evaluation, research,
publication
21
Issues
- You must have staff who have energy to reach out
- You must avoid the Exclusive Service mentality
- we exclude everyone who does not meet DSM4
criteria
22
Every minute you take away from a clinician doing
best quality clinical work wrecks any attempt to
provide efficiency.
23
Sustainable Service Development South Australia
- Southern CAMHS (Flinders Medical Centre - 15
years) - 2 teams to 6 teams
- No rural service, to 3 rural teams
- 12 therapists to 40 therapists
- No teaching, to Masters level programs
- No research, to 22 programs including two
longitudinal programs - CHASP Accreditation 1994 (the first CAMHS ever)
- Gold Award THEMHS 1994
24
Clinical Work 1985
- Systematised interviewing (Eisen Irwin)
- 4 sessions of assessment with an initial
interview with the family, then two interviews
with the child, then a family feedback session. - The problem was that the mean number of sessions
attended was only 3, with a mode of 1.
25
Clinical Work 1995
- We reviewed 200 clients to see what had happened
to them. - 50 had got what they wanted
- 20 felt the service had little to offer their
problem
26
Clinical Work 2008Initial Consult System
- Single session
- Asked the patients what they wanted to achieve by
the end of the session - Listed their problems and ranked them
- Discussed alternatives for change in the most
pressing problems - Psychoeducational approach
- Checked at the end of the session to see whether
they had got what they wanted
27
Window Shopping is OK!
28
Registration as a Case
- Genuine issue here
- Do you register at the first session - even if
they are never going to come back? - Or do you wait until they commit to some specific
course of therapy
29
Sustainable Service Development Queensland (2001-
)
- RCH District CYMHS
- Since 2001, Service to BYDC
- CYFOS Development
- MHATODS Team
- Therapy supervision
- Reworking of CL Team and after hours service
- EI Strategy - KOPING strategy
- Recent ACHS Accreditation, exceeding most
standards - Publications (35 per annum - only 7-10 mine)
- Silver THEMHS award 2006
30
RCH Brisbane North CYMHS
- We monitor clinical and other activity, and
provide feedback to staff on a regular basis
through team leaders - We are meeting ALL of the criteria in the
National Workforce Standards documents
Recommended
CrystalGraphics Presentations





























