
Initial Treatment in Parkinson Disease
1 / 19
Title:
Initial Treatment in Parkinson Disease
Description:
LW, a 89 yo female ex-nurse assistant, is a new patient in clinic. ... Physical Therapy, Exercise, Nutrition ' ... How does the harm of therapy compare to benefit? ... –
Number of Views:47
Avg rating:3.0/5.0
Title: Initial Treatment in Parkinson Disease
1
Initial Treatment in Parkinson Disease
- Journal Club
- January 23, 2002
- Megan Mahoney
2
Parkinson Disease A Primary Care Problem
- There are more than 1 million persons in the
United States with PD - More than 50 of patients with PD are treated by
their PCP - The general health of patient with PD is our
responsibility after referral to specialist.
3
Case Presentation
- LW, a 89 yo female ex-nurse assistant, is a new
patient in clinic. Her daughter, who is her
primary caregiver, reports worsening loss of
balance and decreased facial expression
beginning approximately 9 months ago. On ROS, pt
endorses constipation and fragmented sleep. In
general, the patient is an elderly African
American women well-groomed with masked facies
and expression-less, muffled speech. On exam,
mild hand tremor at rest is present bilaterally.
Profound bradykinesia is present, along with
muscular rigidity bilaterally. Sensory exam is
normal.
4
Cardinal features of Parkinson Disease
- Tremor
- Akinesia or bradykinesia
- Rigidity
- Postural instability
- Possible PD
- 1 of the first three listed
- Probable PD
- 2 of the four listed
- (or 1 of first three if asymmetric)
- Definite PD
- 3 of the four listed
5
Associated features of PD
- Motor
- Hypophonia
- Dysphagia
- Shuffling gait
- Masked facies
- Sensory
- Pain
- Paresthesia
- Autonomic dysfunction
- Constipation
- Urinary dysfunction
- Thermal dysregulation
- Seborrhea
- Psychiatric manifestations
- Sleep disturbances
6
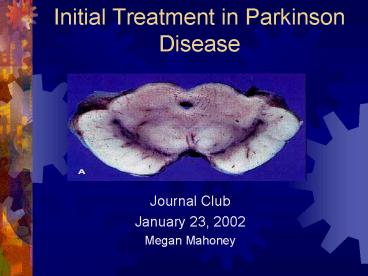
Therapeutic options for PD
- The motor symptoms of idiopathic PD are primarily
the result of a progressive loss of
dopamine-containing neurons in the substantia
nigra. The midbrain above shows the normal
pigmentation of the substantia nigra. The lack of
pigmentation, seen below, is from a person with
Parkinson disease.
7
Levodopa
- Side Effects
- Nausea/Vomiting
- Orthostatic hypotension
- Psychological side effects
- Wearing off periods
- Dyskinesias
- Precursor to dopamine
- Crosses BBB
- Combine with Carbidopa to block peripheral
conversion
8
Dopamine Receptor Agonists
- Side effects
- Orthostatic hypotension
- Hypersomnolence
- Hallucinations
- Nausea/Vomiting
- Adjunctive medication to reduce dyskinesias
secondary to levodopa - Bromocriptine, Pergolide, Pramipexole, Ropinirole
9
Other Anti-PD Therapies
- Anticholinergics particularly effective in
reducing tremor, rigidity, drooling not in
bradykinesias - Amantindine not as effective as levodopa, can
reduce severity of dyskinesias - MAO-B inhibitors symptomatic benefit
- COMT inhibitors potentiates levodopa
- Vitamin E, Coenzyme Q10, evening primrose
- Physical Therapy, Exercise, Nutrition
10
A Five-year Study of the Incidence of Dyskinesia
in Patients with Early Parkinsons Disease who
were Treated with Ropinirole or Levodopa
11
How was randomization done?
- Participants were randomized 21 ropinirole vs.
levodopa. - Average age was 63 for both groups.
- Duration of disease, severity of disease,
baseline ADLs and motor function scores were
similar between the two groups.
12
Was the study blinded?
- Both clinicians and patients were unaware of
treatment arm assignment. - Both groups were offered supplemental levodopa in
an open label fashion. - There was no follow-up assessment of blinding
after completion of study.
13
Was follow-up of patients long enough to capture
effect?
- Approximately 50 of patients with PD develop
dyskinesias after 3 to 5 yrs of levodopa therapy. - Intention-to-treat model was used to record
incidence of dyskinesia, but not for other
parameters.
14
Are the results valid?
15
Are the results valid?
- Reduced incidence of dyskinesias (hazard ratio
2.82, 95 CI, Plt0.001) - Length of time until dyskinesia in 25 of group
was 214 wks in ropinirole vs. 104 wks in
levodopa.
- At end of study, 20 of ropinorole group
developed dyskinesias vs. 45 of levodopa group. - Only 8 of ropinole group reported disabling
dyskinesias vs. 23 of levodopa group.
16
Are the valid results of this study important?
- Dyskinesia was recorded when patients had a score
1 or more on 0-4 scale. - Dyskinesia was reported as incidence, not
severity. - Incidence of disabling dyskinesia provides more
information regarding severity. - There was no measure done on quality of life.
17
How does the harm of therapy compare to benefit?
- There was a slight worsening from baseline in the
score for ADLs in ropinirole group, which was not
significant. In levodopa group, there was no
change in ADLs. - The increment of improvement in motor function
seen in two groups was significantly higher in
levodopa group.
18
How does the harm of therapy compare to benefit?
- Hallucinations were significantly increased in
ropinirole group with NNH of 8 (compared to NNT
of 4). - Many patients prefer moderate dyskinesias to
bradykinesias and rigidity. - Cost is prohibitive.
19
Bottom Line
- There is evidence to support that initial
treatment with dopamine agonists delays the onset
of dyskinesias, but may be less effective in
treating motor function. - Is the delay in complications worth the cost?
- Dopamine agonists should be avoided in patients
prone to hallucinations and confusion, such as
the elderly.
Recommended
CrystalGraphics Presentations





























