
LSUHSC Occupational Therapy Brachial Artery Treatment Protocol - PowerPoint PPT Presentation
1 / 5
Title:
LSUHSC Occupational Therapy Brachial Artery Treatment Protocol
Description:
Below the antecubital fossa it branches into the radial and ulnar artery ... Arterial insufficiency: digits will turn white or pale in color. Postoperative Therapy ... – PowerPoint PPT presentation
Number of Views:195
Avg rating:3.0/5.0
Title: LSUHSC Occupational Therapy Brachial Artery Treatment Protocol
1
LSUHSC Occupational TherapyBrachial Artery
Treatment Protocol
Carla Saulsbery LOTR,CHT Dr. A. Hollister MD
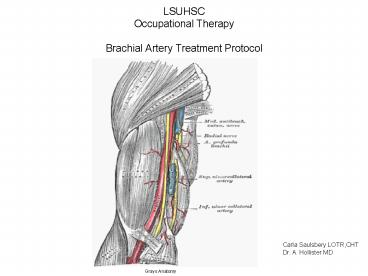
Grays Anatomy
2
- Brachial Artery has three main branches. The
profunda brachi is the first and - most important
- Below the antecubital fossa it branches into
the radial and ulnar artery - Commonly injured from both penetrating and
blunt trauma usually associated - with humeral fractures. At greatest risk in
proximal one- third, where it - lies next to the humeral shaft, and in the
distal one-third near the elbow. - After cardiac catheterization 1.5 of patients
require thrombectomy - Repair by end to end anastomosis or saphenous
vein graft - Any hematoma may compress the brachial artery
or median nerve in the - antecubital fossa and result in ischemia or
neuropathy or both - The greatest amount of healing in the vascular
system occurs within the first - four weeks.
- Healing of the endothelial lining occurs within
the first 2 weeks. - Remobilization is initiated after endothelial
healing has occurred. - Injury to the brachial artery will cause
radiating pain, decreased skin - temperature, decreased pulses and pallor of
the distal arm and may result - in Volkmann contracture
3
- Precautions
- Follow precautions identified from the surgeon
regarding specifics of the - vessel repair
- Extremes in temperature which could cause
vascular spasm. - Arterial spasm can lead to ischemia
- Avoid excessive external compression from
dressing splints, etc. - Therapy is not indicated when there is
thrombosis or vessel integrity - is in question.
- Pain from vigorous exercise may precipitate
vasospasm - Activity or splints should not decrease digital
temperature. - When removing dressing avoid trauma to the soft
tissues which could lead - to vascular spasm.
- Arterial insufficiency digits will turn white
or pale in color.
4
- Postoperative Therapy
- 0-2 weeks
- Elevation of the extremity. Flex elbow 60-90.
Begin elbow flexion exercises. Keep arm in sling
or fabricate LA splint - Splint to the hand and wrist as needed to
decrease edema, preserve the arches of hand.
Preserve ligament length - AROM exercises to the shoulder and hand
- Patient education in avoidance of caffeine,
temperature extremes - Watch for signs of vascular compromise-may
include increase edema, - decreased temperature, or increased pain.
- 3 weeks post op
- Gentle AROM exercises to the elbow and wrist in
extension and flexion - Baseline sensory and motor exam of median nerve
as indicated - Address joint tightness, soft tissue tightness
adhesion prevention, - sensory dysfunction
- 5 weeks post op
- Once vascularity is stabilized light compression
can be started - Retrograde massage
5
- Weeks 6-8
- Light functional activities
- Pressure garments if no signs of infection or
vascular instability - Scar management
- Weeks 8-10
- Light resistive and progressive strengthening as
tolerated - Sensory re-education as indicated
Recommended
CrystalGraphics Presentations





























