
Accumetrics VerifyNow - PowerPoint PPT Presentation
1 / 24
Title:
Accumetrics VerifyNow
Description:
Light transmittance (activated platelets will aggregate beads leading to increased light) ... The beads can degrade after prolonged exposure to room air ... – PowerPoint PPT presentation
Number of Views:623
Avg rating:3.0/5.0
Title: Accumetrics VerifyNow
1
Accumetrics VerifyNow
2
Outline
- Review of platelets and thrombosis
- How does Aspirin/Plavix work
- How does the test work
- What is Aspirin/Plavix resistance
- How will the test be used clinically
- Limitations
3
What are we trying to do?
4
Formation of platelet plug
5
What do activated platelets look like?
EM of dormant platelets
Activated platelets
6
How do you activate platelets?
7
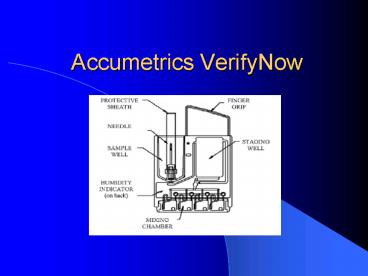
Basic principle of test
- Incubate the following
- Human fibrinogen-coated beads
- Platelet agonist
- Buffer and Preservative
- Anticoagulated (3.2 Citrate) Blood sample from
patient - Measure
- Light transmittance (activated platelets will
aggregate beads leading to increased light)
8
VerifyNow Aspirin Test
- Agonist is Arachidonic Acid
- Report results as
- gt 550 ARU (Aspirin Reaction Units) No platelet
disfunction - lt 550 ARU Platelet disfunction consistent with
aspirin - Results should be interpreted with other
laboratory and clinical data available to the
clinician.
9
Expected Values
10
Test limitations
- The beads can degrade after prolonged exposure to
room air - Patients with inherited (i.e. VWD) or acquired
platelet disorders have not been studied - Patients receiving other antiplatelet agents may
not be tested (GPIIb/IIIa inhibitors, Plavix,
Motrin)
11
P2Y12 Assay
- Instead of Arachidonic Acid, use ADP
- As a control for baseline platelet function, have
a separated channel with iso-TRAP (Thrombin
Receptor Activating Peptide) and
fibrinogen-coated beads. - Report P2Y12 Reaction Units (PRU)
- Inhibition (Base PRU) x 100
- Base
- Results in no interference with Aspirin, other
NSAIDS.
12
Expected values
13
GPIIb/IIIa Assay
- Use iso-TRAP as activator (Thrombin Receptor
Activating Peptide) - Reports as Platelet Aggregation Units (PAU)
- No interference from aspirin, Plavix, heparin,
warfarin, NSAIDs
14
1/5 Americans uses Aspirin
15
Why is Aspirin recommended?
16
Coronary Events after Stenting
17
New evidence suggests that for many Americans
taking aspirin, the pills do little if any good.
Recent studies have found that anywhere from
5-40 of aspirin users are nonresponsive or
resistant to the medicine. That means that
aspirin does not inhibit their blood from
clotting, as it is supposed to do.
18
Variability in Aspirin response
19
So what?
20
136 patients for elective PCI, using VerifyNow
Assay
21
In summary
- ?Aspirin/Plavix responders seem to do better with
therapy than nonresponders?
22
Mechanisms for Resistance
- Non-compliance or failure to prescribe
- Low absorption (Plavix)
- Variation in liver enzymes (P450-3A4) that
metabolize drugs (Plavix) - Interaction with other drug (Aspirin and Motrin,
statins and Plavix) - Genetic polymorphisms (COX-1, P2Y12,vWF)
- Platelet hyper-reactivity
- Increased norepinephrine
23
Possible Uses
- Educate patient on importance of compliance
- Eliminate interfering medication (ibuprofen)
- Increase dose
- Switch medication
- Help decide whether someone on Asprin/Plavix is
safe to go to the OR (assess risk of bleeding)
24
Remaining Problems
- Various definitions different criteria/methods
-gt wide range (5-40) - How stable is this phenomenon over time?
- Are there specific populations at risk (women,
diabetics)? - What is the best test (Optical platelet agg,
VerifyNow, PFA-100, Bleeding time, urinary
thromboxane)??? - What is the clinical approach to Aspirin/Plavix
resistance? - Will this lead to more lives saved?
Recommended
CrystalGraphics Presentations





























