
Assessment of the MusculoSkeletal System - PowerPoint PPT Presentation
1 / 25
Title:
Assessment of the MusculoSkeletal System
Description:
Apply knowledge of Anatomy and physiology of musculoskeletal system ... The fact is, without muscles, you wouldn't be alive for very long ... – PowerPoint PPT presentation
Number of Views:3269
Avg rating:5.0/5.0
Title: Assessment of the MusculoSkeletal System
1
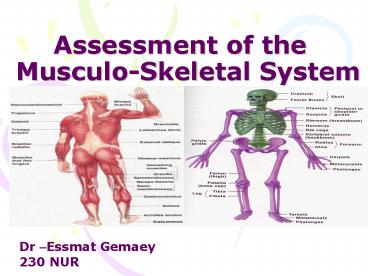
Assessment of the Musculo-Skeletal System
Dr Essmat Gemaey 230 NUR
2
Outlines
- Review of Anatomy and physiology of
musculoskeletal system - Physical Exam
- Inspection
- Palpation
- ROM (Rang of motion)
3
Objectives
- Apply knowledge of Anatomy and physiology of
musculoskeletal system - Differentiate between normal and abnormal
- Implement physical assessment
4
(No Transcript)
5
What do muscles do ?
- Muscles simply move you!
- Without muscles you couldn't open your mouth,
speak, shake hands, walk, talk, or move your food
through your digestive system. - There would be no exploring, running, climbing,
smiling, blinking, breathing. You couldn't move
anything inside or outside you. The fact is,
without muscles, you wouldn't be alive for very
long
6
(No Transcript)
7
- The skeleton is the name given to the collection
of bones that holds our body up. - Our skeleton is very important to us. It does
three major jobs. - 1. It protects our vital organs such as the
brain, the heart, and the lungs. - 2. It gives us the shape that we have. Without
our skeleton we would just be a blob of blood and
tissue on the floor. - 3. It allows us to move. Because our muscles are
attached to our bones, when our muscles move,
they move the bones, and we move
8
Physical Exam
- Inspection
- Observe any lack of symmetry and any evidence of
trauma or disease. - Look for muscle wasting
- Inspect the joint contour (shape) and observe
any evidence of swelling, deformity or
inflammation.
9
- Ask the client to point to, or otherwise
identify, any painful areas, including sites of
radiation of - pain.
- Screening questions for musculoskeletal
disorders - 1. Do you have any pain or stiffness in your
arms, legs or back?2. Can you walk up and down
stairs without difficulty?3. Can you dress
yourself in everyday clothes without any
difficulty?
10
- Assessment of Gait
- Ask the patient to walk back and forth across the
room. - Observe for equality of arm swing , balance and
rapidity and ease of turning. - Next, ask the patient to walk on his tiptoes,
then on heels. - Ask the patient to tandem walk.
- Test patient's ability to stand with feet
together with eyes open and then closed.
(Romberg's test). Reassure patient that you will
support him, in case he becomes unsteady. - Normal Person can walk in balance with the arms
swinging at sides and can turn smoothly. Person
should be able to stand with feet together
without falling with eyes open or closed.
heels
tiptoes
tandem
11
Upper Extremity Muscles
- Inspect the muscles of the shoulder, arm, forearm
and hand. - Note muscle size (bulk).
- Look for asymmetry, atrophy and fasciculation.
- Look for tremor and other abnormal movement at
rest and with arms outstretched.
12
Determine muscle power by
- Gently trying to overpower contraction of each
group of muscles. - Shoulder Abduction (Deltoid)
- , Adduction
- , Shrug (Trapezius)
Abduction
Adduction
Trapezius)
13
- Elbow flexion (Biceps)
- Elbow extension (Triceps)
- Wrist Flexion ( )and extension().
14
- Hand Grip
- opposition of thumb and index finger
- opposition of thumb and little finger and
- finger abduction and adduction.
Grip
15
- Determine limb tone (resistance to passive
stretch). - With the patient relaxed
- Gently move the limb at the shoulder, elbow and
wrist joints and note whether tone is normal,
increased or decreased
16
Normal findings
- Muscles are symmetrical in size with no
involuntary movements. - In some, muscles may be slightly larger on the
dominant side. - Muscle power obviously varies. You should not be
able to overpower with reasonable resistance. - You have to learn to appreciate the normal tone
from practice.
17
Neck Range of Motion of
- Fix the head with one hand while you examine neck
- Inspection
- Note the normal concavity of cervical spine
- Identify Transverse process of C7
- Observe Trapezius and Sternomastoid muscles
- Palpation
- Feel each spinous process looking for focal areas
of tenderness - Joint
- Feel for crepitus during passive motion
- Para spinal muscles
- Range of motion
- Active
- Touch chin for flexion
- Throw head back for extension
Touch chin
Throw head back
18
- Touch each shoulder with ears for lateral flexion
- Touch each shoulder with chin for lateral
rotation - Passive
- Feel for crepitus during passive motion
- Normal
- 30 degree rotation, able to touch chest with
chin, 55 degree extension and 40 degree lateral
bend. - No resistance during the range of motion.
19
Muscles of Lower Extremity
- Inspect the muscles of the hip, knee and ankle.
- Note muscle size (bulk).
- Look for asymmetry, atrophy and fasciculation.
- Look for abnormal movement.
- Determine muscle power by gently trying to
overpower contraction of each group of muscles. - Hip Flexion (Iliopsoas), Extension (Gluteus
maximus), Abduction, Adduction.
Hip flexion
20
The Knee Exam
- Inspection
- Make sure that both knees are fully exposed. The
patient should be in either a gown or shorts.
Rolled up pant legs do not provide good exposure!
- Watch the patient walk.
- Do they limp or appear to be in pain?
- When standing, is there evidence of bowing
(varus) or knock-kneed (valgus) deformity? There
is a predilection for degenerative joint disease
to affect the medical aspect of the knee, a
common cause of bowing.
varus Knee deormity, more marked on the left leg
21
- Is there evidence of atrophy of the quadriceps,
hamstring, or calf muscle groups? Knee
problems/pain can limit the use of the affected
leg, leading to wasting of the muscles.
While both legs have well developed musculature,
the left calf and hamstring are bulkier than the
right
22
- Knee Flexion (Hamstrings), Extension
(Quadriceps) - Ankle Dorsiflexion (Tibialis anterior), Plantar
flexion (Gastronemius). - Determine limb tone resistance to passive
stretch. With the patient relaxed, gently move
the limb at the hip, knee and ankle and note
whether tone is normal, increased or dicreased.
Flex the hip and knee. - Support the knee, dorsiflex the ankle sharply and
hold the foot in this position checking for
clonus.
Knee extension
Knee flexion
Dorsiflexion
23
Spine (Bone)
- The examiner should stand behind the patient and
observe the alignment of the spine in the flexed
position to determine scoliosis. - View the spine from the side to determine
kyphosis. - Ask the patient if he is aware of sore spots.
Palpate the spinous process and be gentle with
the sore spots. Percuss one vertebra at a time,
starting from head. - .
24
- Assess range of motion of spine by having patient
bend down to pick up an object without bending
his legs while you hold his hips. - Normal
- Gentle concavities in cervical and lumbar regions
and a convexity in the thorax. - Vertebral line and gluteal cleft align
25
Thank you
Recommended
CrystalGraphics Presentations





























