
GENERAL HOSPITAL - PowerPoint PPT Presentation
1 / 32
Title:
GENERAL HOSPITAL
Description:
Children and Young Peoples Centres. Focusing on the Family and preventive health. ... Health visitors, dentists, pharmacy, a cardiology clinic, x ray facilities, ... – PowerPoint PPT presentation
Number of Views:167
Avg rating:3.0/5.0
Title: GENERAL HOSPITAL
1
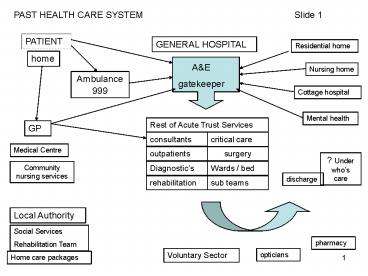
PAST HEALTH CARE SYSTEM
Slide 1
PATIENT
GENERAL HOSPITAL
Residential home
home
AE gatekeeper
Nursing home
Ambulance 999
Cottage hospital
Mental health
Rest of Acute Trust Services
GP
consultants
critical care
Medical Centre
outpatients
surgery
? Under whos care
Wards / bed
Diagnostics
Community nursing services
discharge
rehabilitation
sub teams
Local Authority
Social Services Rehabilitation Team
pharmacy
Voluntary Sector
opticians
Home care packages
2
THE PAST
Slide 2
- Scoop and run ambulances
- Admit to assess need and treatment
- Large uncontrolled demand which is unscheduled
and urgent - Inappropriate use of AE patients with alcohol,
drug and mental health issues which cannot be
dealt within the hospital environment - Overcrowded, understaffed, under-resourced
casualty departments - Trolleys
- Sickest patients seen by most junior doctors
- Patchy primary care
- FRAGMENTATION
3
The Future Vision 2008 HEALTH CARE SYSTEM
Slide 3
Ambulance Trust
General Hospital
AE
999
ECP
No AE
NHS Direct
Complex surgery
Super GP Surgeries
Community Hospital
Urgent Care Unit
Urgent Care Centres
PATIENT HOME
Minor Surgery
W I C
ESS
EMS
Diagnostic Tests
Acute Alcohol Team
MIC
Outpatient Clinics
PCC
Rapid Response Team
ECP
Well Being Clinics
Acute Substance Abuse Team
I S T C
Long Term Conditions Clinics
Local Authority
Low Vision Services
Rehabilitation Team
Voluntary Sector
pharmacy
opticians
4
KEY TO FUTURE VISION OF HEALTH AND SOCIAL CARE
SYSTEM 2008
Slide 4
- WIC Walk in Centres
- MIC Minor Injuries Centres
- ESS Emergency Social Services Team
- EMS Emergency Mental Health Team
- ECP Emergency Care Practitioner
- ISTC Independent Sector Treatment Centres
- PCC Primary Care Centre
Patient self referral
Practitioner referral
Dashed box indicates service sits in community
and is co-located with other services in one
site. This depends on model adopted by PCT
Increase in the type and access to urgent care
services in the community Principle is to assess
need before admission. Treat in the field nearer
to home. Reflecting the closure in AE
Departments. More choice, easier to access, more
convenient, improved quality of care, faster
care. Services are centred around the patient.
5
THE SERVICE IN 2008
Slide 5
- PATIENT FOCUSED
- Community centred
- Care close to home where possible
- Simple access
- Seamless pathways
- High quality
- CONTROLLED DEMAND, planned surgery and admission
to Independent Treatment Centres or Super
Sugeries - Offers choice
- Encouraging all health partners to work together
in a system-wide approach to developing urgent
care services
6
The Future Vision 2008 Introduction of New
Models of Service Delivery
Slide 6
- New Health Surgeries
- Increased investment into GP Practices giving
rise to new - Health Centres, Polyclinics, Super Surgeries,
or Primary - Care Centres.
- 125 such centres to open by December 2006,
outside general hospitals, by 2008 the total will
be 750 units - Offering a wide range of services under one roof.
The services provided will reflect the needs of
the locality. This should be achieved through the
PCTs understanding the needs of their population
through research evidence and consultation with
service users about want they want.
7
Slide 7
- GPs with specialist interests and Consultants
e.g. ophthalmology, - community nurse, district nurses, midwifery,
dentistry, - physiotherapy, pharmacy, optometry,
podiatry. - Management of long term conditions such as
Diabetes, Heart - Disease, Elderly Care, Asthma, Well being
clinics, Outpatient - Clinics and wide range of diagnostic tests.
- To facilitate this budget control has been
transferred from national - control to local level.
- 5 of the NHS budget has been transferred from
the Acute Trust - (general hospital) to the PCTs. This means
PCTs and GP hold the - purse strings to commission or provide
services, they deem - appropriate.
8
- New Community Hospitals
- Will offer patients wide range of access to
health and social care which will be co-located
on the same site. They will complement the
specialist general hospital, providing speedy
access to key medical tests, day case and
outpatient surgery. They will be integrated with
Social Service Departments. - providing care closer to home in six specialities
ear, nose and throat,
trauma and orthopaedics, dermatology, urology,
gynaecology and general surgery. - 700 million into new buildings through NHS LIFT,
by the end of 2005, 54 new buildings were opened
and in 2006, a new LIFT building is expected to
open every week. - Purpose-built facilities, where GP services are
on the same site as pharmacies and social
services, The centres are more convenient for
patients, particularly older patients and those
with long-term conditions, as they offer more
care closer to home. - some models of community hospitals will provide
Urgent Care Units
Slide 8
9
Examples of Community Hospital Developments
Slide 9
Reference to CISP, 2006 Developing Community
Hospitals Models of ownership 1 pdf, gives
cases of community developments of
hospitals. Recommended referencing to the Funding
Team as it explains how voluntary organisations
can fund services from the NHS.
10
Slide 10
- Services which may be provided in Community
Hospitals - Long term conditions Clinics
- a resource Base for management of LTC with
Specialist GP interest and Consultants for
chronic disease management in the community. - Older people
- Multidisciplinary Assessment Centre, for falls /
mobility and complex needs. Integrating
intermediate, social, urgent care and mental
health. - step- up / down intermediate care
- In / out patient clinics for comprehensive
assessment for long term packages of care. - Children and Young Peoples Centres
- Focusing on the Family and preventive health.
Based on integrated and co-ordinated care across
wide selection of agencies. Plan is for 3,500
Childrens Centres by 2010.
11
- Service which may be provided in Community
Hospitals - Self Care and Self Management
- The following facilities will be provided to
enable self care of own health - Education Rooms for Action on Personal Health
- terminals for personalised support packages for
lifestyle changes, - rooms to meet with health trainers and personal
advisors - gym equipment, yoga, dance, drama and music
facilities - kitchen facilities for cooking and learning new
skills - Facilities fpr Self Assessment
- enabling an individual to complete own health
check - enable to check own blood testing, borrow, learn
and use self testing equipment. - Facilities for Information Encompassing
- provision of both general and local information
- enabling individuals to obtain help and learn
how to access it and how to personalise it. - Sign posting
Slide 11
12
Service which may be provided in Community
Hospitals Mental Health Facilities The
principles of Self care and self management
extends to Mental Health Services. Priorities
focus on the development of community Well-being
Resource Centres providing services and access to
agencies in community locations e.g. Employment
Advisers increased uptake of Direct Payments
and advance directives, will enable service users
to receive services in more local facilities
more culturally specific services, contact points
and information services and better use of
community facilities to provide information
signposting on mental health and mental health
services. Our health, our care, our community
investing in the future of community hospitals
and services, 2006) p 40
Slide 12
13
Slide 13
Super surgeries The NHS Plan (2000) describes a
vision of the new GP surgery as, many of the
GPs will be working in teams from modern
multi-purpose premises along side nurses,
pharmacists, dentists, therapists, midwives and
social care staff. Nurses will have new
opportunities and some GPs will tend to
specialises in treating different conditions. An
increasing number of consultants will take
outpatient sessions in local primary care
centres. PCTs are being encouraged to set up
one-stop health centres which bring services,
such as GP. Health visitors, dentists, pharmacy,
a cardiology clinic, x ray facilities, optometry
services, Sure Start and healthy living café
under one roof. Work on about 50 centres is
underway. (The NHS in the UK 2006/07)
14
An acute hospital admission is a failure of the
Health System.
Slide 14
- The real challenge to the NHS is how to manage
chronic disease better
15
Slide 15
URGENT CARE is all unscheduled, urgent and
emergency care, i.e. anything which is not a
programmed activity
Current Admissions - 70 elderly, Majority with
long term conditions of which 50 are
unnecessary.
- The 20 of Patients who need 80 of the Care
- Older People
- Decreased Functional Ability
- Mobility, sight loss, daily living skills
- Revolving Door Admissions
- COPD Heart Failure
- End of Life
- Psychological Social Support
- Packages of care tailored to the individual
16
Slide 16
- Urgent care Services
- Our health, our care, our community investing
in the future of community hospitals and
services, 2006) p 40 states, - Community Hospitals have a future major role in
Urgent and Unscheduled care. - It anticipates an increase in this type of
provision which will be set out in future
government Urgent Care Strategy. - Minor injury units (MIU) and NHS Walk in Centres
(WIVs) are providing much urgent / unscheduled
care in the community. - A network of Urgent Care Centres are planned
which will be nurse led and co-located with out
of hours GPs, emergency social services team and
emergency mental health teams, ambulance base
with Emergency Care Practitioners (ECP) - Central will be Diagnostic Facilities, X-Rays for
example will prevent unnecessary attendances to
acute general hospitals. - Urgent Care Centre will additionally act ( in
some models of practice) as a resource for
management of chronic disease.
17
Slide 17
- The Urgent Care Strategy
- The new focal point for integrated unscheduled/
urgent care - URGENT CARE PLUS
- The link to Long Term Conditions (LTC)
- Base for community matrons
- LTC diagnostics
- LTC review clinics
18
our health, our care, our community
investigating in the future of community
hospitals and services (DOH, 2006)
Slide 18
- A new generation of community hospitals and
services - The White paper defines what a community
hospitals and services are as covering the
following - The broad range of services that are sited in
defined local - communities with small populations rising to
about - 100,000
- Any clinical or social care functions that can
be provided safely - and appropriately away from large specialist
centres and those - services and functions that benefit from close
links to other local - services, for example intermediate care
services aimed at enabling an - older person to regain independence in their
own home . - Will not undertake complex surgery requiring
general anaesthetic nor - provide fully fledged accident and emergency.
- It means that some larger hospitals will
concentrate on specialist - services and some will merge or close
19
Individual and Community Oriented Preventative
Action for Health
Slide 19
Individually oriented preventative action
Health Hazards
Environmental hazards
Community oriented preventative action
poor education
poor food nutrition
unemployment
poor housing
poverty
Intersectoral action for Health. WHO. 1986
20
Delivering Choosing Health (DOH 2004)
Slide 20
- Key messages
- Making healthy choices easy choices
- Interventions for the disadvantaged
- Health policy to inform and support
- Principles
- Informed choice
- Personalisation supporting people to make
healthy choices, especially deprived groups and
communities - Working together through effective
- Choosing Health priorities
- Reducing health inequalities
- Reducing smoking, obesity, alcohol consumption,
- Tacking hypertension, poor dietary intakes, lack
of exercise, - Improving mental health and well being
21
Slide 21
22
Slide 22
Level 3
Patients with highly complex needs and
co-morbidities
Case management
Disease management equally shared care
Level 2
High risk patients
Level 1
Largely self care
70-80 population
23
Future Health Care Trends an overview
- There are many powerful forces for change in our
populations health and the way we deliver health
care. - The population is ageing. The balance between
young and old is shifting. Life expectancy is
increasing, as premature mortality rates fall.
The average family size of 1.77 (2004) sits below
the replacement level of 2.1. The number of
single person and single parent households is
growing. The number over 60 are expected to grow
by nearly a third by 2021, while the numbers of
young people under 16 will fall. The ethnic
population is also ageing. However, there is
significant uncertainty about the net impact of
the ageing population on health care demand.
24
- The workforce is changing and ageing. The
national and international competition for
skilled staff will grow. The workforce is
demanding a better work/life balance. - Current lifestyles present major risks to the
future health of the population. Obesity,
sedentary lifestyles, sexually transmitted
disease, and alcohol consumption are growing,
especially amongst the young. This is driving
increased incidence in diabetes, osteoarthritis,
heart disease and kidney disease. Over a quarter
of the population still smoke. This creates a
significant burden of respiratory disease and
cancer. - Health inequalities continue to present a
challenge. People from lower socio-economic
groups are much more likely to adopt risk taking
lifestyles and yet are frequently handicapped in
accessing health services and taking on board
positive health messages - 40 of those from
social classes DE have poor literacy skills.
25
- The disease profile is changing. Previously fatal
acute conditions such as cancer and heart disease
can now be treated. Ageing related and chronic
diseases, such as diabetes, respiratory illness,
renal disease and arthritis, are becoming much
more significant. More people are living with
long term illness, and with multiple conditions. - Medical advance can improve health outcomes, but
will create budgetary pressures. Significant
advances in medicine and surgery are anticipated,
supported by the increasing insight offered by
genetics. The capacity to treat is increasing,
especially the older frail. This magnifies the
potential demand of an ageing population. - The expectations of society are changing. Rising
education and income levels are helping to drive
higher public expectations of health and health
care services. The future old are expected to be
much more demanding than their current
counterparts.
26
- Advances in information technologies enable
improved models of care. The capacity to share
clinical information and expertise between
professionals and patients offer many
opportunities for patients to take a positive and
active role in their care and improve the
quality of patient care and outcomes. - These forces bring threats and opportunities to
the health of the population and health care
services. The impact on health care demand and
our capacity to meet that demand is very
difficult to foretell. - There is significant debate about the impact of
an ageing population. The incidence of chronic
disease grows markedly in those over 60, but
there is also evidence that the old of today are
fitter than the old twenty years ago, postponing
the onset of chronic disease. As chronic
conditions are diagnosed earlier, treatment is
likely to be more effective. One of the greatest
uncertainties is that of the impact of current
lifestyles on the population over the next two
decades. Will the young of tomorrow have even
greater levels of obesity, sexually transmitted
disease and drug misuse than the young of today,
and will the old be sicker and more dependent? A
lot will depend on societys attitude and
response to risk taking behaviours. We have the
opportunity to live longer and healthier lives
than ever. Will society grasp that opportunity,
or will we see health inequalities increase as
some do and some dont, or perhaps cant.
27
Large growth in the number of older people what
will be the impact on total health care costs?
Per capita costs are greater for older people
- Starting from 2006, the post-war baby boom will
boost the year-on-year growth rates in the
elderly populations, with growth rates peaking in
2012. - The number of people over 65 is expected to grow
by - 527,000 - 2010
- 1,619,000 2015
- 2,390,000 - 2020
Hospital and community health service expenditure
by age of recipient ( per head, 2002/03)
Source DH
28
An increased capacity to treat and reduced age
discrimination are raising intervention rates in
older people
Demographics and Medical Demand ( increase,
1990-2000)
(1)
- Coronary Artery Bypass Grafts
- Source DH, ONS
29
New technologies offer a means to bridging the
care gap
New technologies enable a different relationship
with older service users
- Social Care is developing a number of new care
models - Extra care housing
- Homeshare
- Adult placement
- Technology-enabled services
- Connected care centres
30
(No Transcript)
31
The Planning FrameworkIt outlines four
objectives for the future NHS
32
Our health, our care, our say
- People want to keep themselves well, and take
control of their own health. They wanted more
help through - Better information
- Advice
- Support
Recommended
CrystalGraphics Presentations





























