
kidney disease
Title:
kidney disease
Description:
medicine –
Number of Views:11026
Title: kidney disease
1
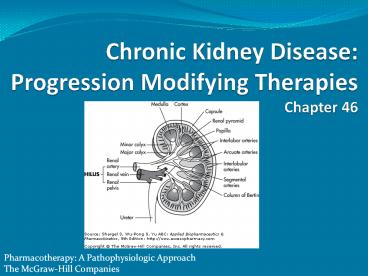
Chronic Kidney Disease Progression Modifying
Therapies Chapter 46
Pharmacotherapy A Pathophysiologic Approach
The McGraw-Hill Companies
2
Abbreviations
ACEI angiotensin-converting enzyme inhibitor
ARB angiotensin receptor blocker
CCB calcium channel blocker
CKD chronic kidney disease
DCCT Diabetes Control and Complications Trial
ESRD end-stage renal disease
GFR glomerular filtration rate
HMG-CoAß-hydroxy-ß-methylglutaryl coenzyme A (reductase)
IIT intensive insulin therapy
K/DOQI Kidney Dialysis Outcomes and Quality Initiative
MAP mean arterial blood pressure
MDRD Modification of Diet in Renal Disease
NHANES III Third National Health And Nutritional Examination Survey
USRDS United States Renal Data System
3
Key Concepts
- Chronic Kidney Disease (CKD) US Prevalence
- 19 million
- The Kidney Disease Outcomes Quality Initiative
(K/DOQI) - CKD risk factor categories
- susceptibility factors
- initiation factors
- progression factors
4
Key Concepts
- Mechanisms of CKD progression
- reduction in kidney mass
- glomerular hypertension
- intratubular proteinuria
- 5 CKD stages based on
- structural damage
- renal function
5
Key Concepts
- Serum creatinine (SCr)
- unreliable marker of kidney function in select
patients - elderly
- malnourished
- children
- estimate GFR
- used to evaluate rate of disease progression
6
Key Concepts
- Stage 5 CKD symptoms
- asterixis
- pruritus
- dysgeusia
- nausea, vomiting
- anorexia, weight loss
- susceptibility to bleeding
- Signs/symptoms of uremia foundational to decision
to implement kidney replacement therapy
7
Key Concepts
- Titrate ACEI/ARB to maximal suppression of
urinary albumin excretion for DM patients with
persistent microalbuminuria despite intensive
insulin therapy - even without HTN
- ACEIs/ARBs key pharmacologic treatments
- hemodynamic BP reduction effects limit kidney
- disease progression
8
Key Concepts
- Supportive therapies may slow CKD progression
- dietary protein restriction
- lipid-lowering medications
- smoking cessation
- anemia management
- Limit progression with hyperglycemia HTN
treatment
9
Epidemiology
- Worldwide public health problem silent epidemic
- CKD affects 5 of adult US population
- CKD defined as SCr gt 1.2 to 1.5 mg/dL
- The Third National Health And Nutritional
Examination Survey (NHANES III) - nationally representative sample of US adult
population - gt 10.9 million people have SCr gt 1.5 mg/dL
- CKD prevalence 10.9 of US population age gt 20
yrs (19 million) if microalbuminuria
proteinuria included
Levey AS, Coresh J, Balk E, et al. National
Kidney Foundation practice guidelines for chronic
kidney disease Evaluation, classification, and
stratification. Ann Intern Med 2003139137147.
Jones CA, McQuillan GM, Kusek JW, et al. Serum
creatinine levels in the U.S. population Third
National Health and Nutrition Examination
Survey. Am J Kidney Dis 199832992999.
10
Etiology
- Susceptibility factors
- advanced age
- low income or education
- racial/ethnic minority status
- reduced kidney mass
- low birth weight
- family history
- Useful for identifying populations at high risk
for CKD
11
Etiology
- Initiation factors
- result in direct kidney damage
- modifiable by pharmacologic therapy
- DM, HTN, autoimmune diseases, polycystic kidney
disease, systemic infections, urinary tract
infections, urinary stones, lower urinary tract
obstructions, drug toxicity - Most common causes of CKD in the US
- diabetes mellitus
- HTN
- glomerular diseases
12
Etiology
- Progression factors
- associated with further kidney damage
- evident as increased decline in kidney function
in patients who already have kidney damage - proteinuria, elevated BP, smoking
- Predictors of progressive CKD
- persistence of underlying initiation factors
- DM
- HTN
- glomerulonephritis
- polycystic kidney disease
13
The Kidney
- 2 million nephrons
- filter
- reabsorb
- excrete solutes
- excrete water
- Primary regulator
- Na H2O balance
- acidbase homeostasis
- Hormone production necessary for RBC synthesis
Ca2 homeostasis
14
Pathophysiology
- Heterogeneous causes
- diabetic nephropathy glomerular mesangial
expansion - hypertensive nephrosclerosis kidney's arterioles
have arteriolar hyalinosis renal cysts present
in polycystic kidney disease - initial structural damage may depend on the 1
disease - Progressive nephropathies result in irreversible
renal parenchymal damage ESRD - Key pathway elements
- loss of nephron mass
- glomerular capillary hypertension
- proteinuria
15
(No Transcript)
16
Pathophysiology
- Initiation factor exposure
- remaining nephrons hypertrophy to compensate for
loss of nephron mass and renal function - compensatory hypertrophy may be adaptive
- hypertrophy may lead to intraglomerular
hypertension - possibly mediated by angiotensin II
17
Kidney Disease/Injury
- acute renal failure
- rapid loss of kidney function
- hours to weeks
- 50 increase in SCr (gt 0.5 g/dL)
- chronic kidney disease
- also called chronic renal insufficiency,
progressive kidney disease - progressive loss of function
- months to years
- gradual replacement of normal kidney architecture
with interstitial fibrosis
18
Kidney Disease Classification
- National Kidney Foundation's (NKF) Kidney
Dialysis Outcomes Quality Initiative (K/DOQI)
CKD classification system (stages 1 to 5) - Categories based on structural kidney damage /or
functional changes in GFR for gt 3 months - stage 1 mild structural changes evidenced by
microalbuminuria with "normal" kidney function - stage 5 analogous to end stage renal disease
dialysis or kidney transplantation may be
necessary - increasing number more advanced stage of disease
- SCr inaccurate index of GFR
19
Kidney Disease
- Normal adult kidney function
- GFR 120 mL/min/1.73 m2
- Can diagnose CKD when GFR gt 90 mL/min/1.73 m2
based on - proteinuria
- hematuria
- evidence of structural damage from kidney biopsy
20
CKD Stages
Stage GFRa Prevalencec
1 gt 90b 10,500,000
2 6089 7,100,000
3 3059 7,600,000
4 1529 400,000
5 lt 15d 300,000
a Glomerular filtration rate (mL/min/1.73 m2) b
CKD can be present with normal/near normal GFR if
other markers of kidney disease are present c
Based on elevated albumin to creatinine ratio
dincludes patients on dialysis
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
21
Presentation/Diagnosis
- Development progression may be insidious
- CKD diagnosis
- measure SCr, estimate GFR
- assess urine for protein /or albumin
- CKD stages 3, 4, 5 require additional workup
- anemia
- CV disease
- metabolic bone disease
- malnutrition
- fluid electrolyte disorders
22
CKD Risk Factors
Susceptibility
Advanced age Reduced kidney mass and low birth weight Racial/ethnic minority Family history Low income or education Systemic inflammation Dyslipidemia
Initiation
Diabetes mellitus Hypertension Glomerulonephritis
Progression
Glycemia (among diabetic patients) Hypertension Proteinuria Smoking Obesity
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
23
Diabetes
- Not all individuals with diabetic nephropathy
progress to stage 5 CKD however, high lifetime
risk - Multiple Risk Factor Intervention Trial (MRFIT)
- prospective study
- gt 300,000 individuals screened
- 3 of DM patients develop stage 5 CKD
- DM subjects 12-fold greater RR of stage 5 CKD
- increased risk of nondiabetic CKD causes
- suggests underlying genetic susceptibility
Brancati FL, Whelton PK, Randall BL, Neaton JD,
Stamler J, Klag MJ. Risk of end-stage renal
disease in diabetes mellitus A prospective
cohort study of men screened for MRFIT. Multiple
Risk Factor Intervention Trial. JAMA
199727820692074.
24
Diabetes CKD
- Type 1 DM patients 40 lifetime risk of
developing CKD - Type 2 DM patients 50 lifetime risk of
developing CKD - Greater prevalence of type 2 DM compared to type
1 - 101 ratio in most countries
- majority of CKD due to DM among type 2 DM
patients
Hasslacher C, Ritz E, Wahl P, Michael C. Similar
risks of nephropathy in patients with type I or
type II diabetes mellitus. Nephrol Dial
Transplant 19894859863.
25
Hypertension
- Increases CKD risk
- Exact role as cause/consequence debated
- Kidney has a role in HTN development/modulation
- Generally develops concomitantly with progressive
kidney disease - Early HTN treatment to aggressive goals slows CKD
progression
26
Hypertension
- Multiple Risk Factor Intervention Trial
- 1 prevention
- evaluated effect of an intervention on CHD
mortality - 16 year follow-up
- lifetime risk of stage 5 CKD for patients with
HTN 5.6 - risk varied dramatically by BP
- 0.33 SBP 140 to 150 mm Hg /or DBP 90 to 100 mm
Hg - 4.5 for SBP gt 180 mm Hg or DBP gt 110 mm Hg
Klag MJ, Whelton PK, Randall BL, et al. Blood
pressure and end-stage renal disease in men. N
Engl J Med 19963341318.
27
Hypertension
- Elevated BP increases risk for developing CKD
- Prospective study (n316,675) managed care
patients - increased stage 5 CKD risk in patients with
elevated baseline BP - odds ratio for CKD development
- 2.0 (95 confidence interval CI 1.6 to 2.5) for
SBP 120 to 129 mm Hg DBP 80 to 84 mm Hg
diastolic - 4.3 (95 CI 2.6 to 6.9) for SBP gt 210 mm Hg or
DBP gt120 mm Hg compared to BP SBP lt 120 and DBP lt
80 mm Hg
Perneger TV, Nieto FJ, Whelton PK, Klag MJ,
Comstock GW, Szklo M. A prospective study of
blood pressure and serum creatinine. Results from
the "Clue" Study and the ARIC Study. JAMA
1993269488493.
Hsu CY, McCulloch CE, Darbinian J, Go AS,
Iribarren C. Elevated blood pressure and risk of
end-stage renal disease in subjects without
baseline kidney disease. Arch Intern Med
2005165923928.
28
Glomerulonephritis
- Glomerular diseases initiation factors with
variable epidemiology, pathophysiology - Goodpasture's disease or Wegener's granulomatosus
may progress rapidly to stage 5 cause ARF - Immunoglobulin (Ig) A nephropathy, membranous
nephropathy, focal segmental glomerulosclerosis,
lupus nephritis, others more indolent cause of
CKD - chronic glomerular diseases progress at variable
rates - loss of GFR 1.4 to 9.5 mL/min/year
29
Progression Factors
- Associated with further kidney damage
- Increased rate of kidney function decline in
patients with existing renal dysfunction - Predictors of progressive CKD
- DM
- HTN
- glomerulonephritis
- polycystic kidney disease
- proteinuria
- smoking
30
Proteinuria
- Promotes progressive nephron loss through direct
cellular damage - Filtered proteins toxic to kidney tubule cells
- albumin
- transferrin
- complement factors
- immunoglobulins
- cytokines
- angiotensin II
31
Proteinuria
- Studies demonstrate presence of proteins in renal
tubules activates tubular cells - upregulated inflammatory/vasoactive cytokines
- Associated with complement component activation
on proximal tubule apical membranes - Intratubular complement activation may be key
mechanism of progessive damage - interstitial scarring
- progressive loss of nephrons
- reduction in GFR
32
Smoking
- May promote initiation progression of CKD in DM
patients - Increased rate of CKD progression
- cigarette pack years independent predictive
factor for CKD progression among DM patients - associated with CKD in HTN
- especially among hypertensive black subjects
- studies demonstrate association between smoking,
microalbuminuria stage 5 CKD
Regalado M, Yang S, Wesson DE. Cigarette smoking
is associated with augmented progression of renal
insufficiency in severe essential hypertension.
Am J Kidney Dis 200035687694.
33
Dyslipidemia
- Prevalence increases as kidney function declines
- Characteristic of nephrotic syndrome
- 85 to 90 of patients with decreased kidney
function, proteinuria gt 3 g/day - elevated plasma total low-density lipoprotein
- 50 of patients have low levels (lt 35 mg/dL) of
high-density lipoprotein cholesterol - 60 have triglyceride concentrations gt 200 mg/dL
- Lipid abnormality treatment may slow CKD
progression
Kasiske BL. Hyperlipidemia in patients with
chronic renal disease. Am J Kidney Dis
199832S142S156.
34
Obesity
- Association of obesity with stage 5 CKD
- 47,504 men, 53,249 women 1983 community-based
screening in Japan - BMI associated with increased ESRD men (not
women) - Population-based study
- BMI gt 25 kg/m2 at age 20 years associated with
threefold increase in CKD risk compared to BMI lt
25 kg/m2 - obesity (BMI 30) among men morbid obesity (BMI
35) among women three- to fourfold increased CKD
risk
Iseki K, Ikemiya Y, Kinjo K, Inoue T, Iseki C,
Takishita S. Body mass index and the risk of
development of end-stage renal disease in a
screened cohort. Kidney Int 20046518701876.
Ejerblad E, Fored CM, Lindblad P, Fryzek J,
McLaughlin JK, Nyren O. Obesity and risk for
chronic renal failure. J Am Soc Nephrol
20061716951702
35
Angiotensin II
- May mediate renal disease progression through
nonhemodynamic effects - potent afferent efferent arteriole
vasoconstrictor - preferentially affects efferent arterioles
- increased glomerular capillary pressure,
filtration fraction - intraglomerular hypertension correlates with
systemic arterial hypertension - animal studies demonstrate high intraglomerular
capillary pressure impairs size-selective
function of the glomerular permeability barrier - increased urinary albumin excretion, frank
proteinuria
36
CKD Symptoms
- Generally absent in stages 1 2
- May be minimal in stages 3 4
- General symptoms
- cold intolerance
- shortness of breath
- palpitations
- cramping, muscle pain
- depression, anxiety
- fatigue
- sexual dysfunction
37
Signs of CKD Stages 1 to 4
System Signs of CKD
Cardiovascularpulmonary edema, worsening hypertension, electrocardiographic evidence of left ventricular hypertrophy, arrhythmias, hyperhomocysteinemia, dyslipidemia
Gastrointestinal GERD, weight loss
Endocrine 2 hyperparathyroidism, decreased vitamin D activation, ß2-microglobulin deposition, gout
Hematologic anemia of CKD, iron deficiency, bleeding
Fluid/electrolytes hyper- or hyponatremia, hyperkalemia, metabolic acidosis
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
38
Anemia
- Kidneys secrete 90 of erythropoietin endogenous
hormone necessary for erythropoiesis - Declining kidney function leads to erythropoietin
deficiency anemia - Prevalence of Hgb lt 12 g/dL in patients with GFR
gt 80 mL/min per 1.73 m2 1 to 30
Hsu CY, McCulloch CE, Curhan GC. Epidemiology of
anemia associated with chronic renal
insufficiency among adults in the United States
Results from the Third National Health and
Nutrition Examination Survey. J Am Soc Nephrol
200213504510.
39
Anemia
- Other factors ethnicity, age, gender, blood loss
(particularly in stage 5 CKD) - NKF K/DOQI guidelines recommend evaluating Hgb
levels in all patients with CKD - Prevalence of Hgb lt 12 g/dL increases in stages 3
to 5 CKD
KDOQI Clinical Practice Guidelines and Clinical
Practice Recommendations for Anemia in Chronic
Kidney Disease. Am J Kidney Dis
200647S11S145.
40
Anemia
- Mild anemia can be asymptomatic
- Patients with more severe anemia may experience
fatigue, weakness, shortness of breath - Anemia treatment may improve/resolve symptoms
- may stabilize kidney function
- Early correction of anemia does not reduce CV
risk - Erythropoietin stimulating agents used to correct
anemia
Drueke TB, Locattelli F, Clyne N, et al.
Normalization of hemoglobin level in patients
with chronic kidney disease and anemia. N Engl
J Med 20063552071-84.
KDOQI Clinical Practice Guidelines and Clinical
Practice Recommendations for Anemia in Chronic
Kidney Disease. Am J Kidney Dis
200647S11S145.
41
Cardiovascular Disease
- CKD high rate of CV morbidity mortality
- CKD patients 16 to 37 the life expectancy of
matched population without kidney disease - Epidemiologic study gt 300,000 patients
demonstrated strong relationship between GFR and
CV disease - lower GFR higher incidence of CV disease
- stage 2-4 CKD patients more likely to die from
CV complications than require renal-replacement
therapy
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY.
Chronic kidney disease and the risks of death,
cardiovascular events, and hospitalization. N
Engl J Med 200435112961305.
K/DOQI clinical practice guidelines for
cardiovascular disease in dialysis patients. Am J
Kidney Dis 200545S1S153.
Keith DS, Nichols GA, Gullion CM, Brown JB, Smith
DH. Longitudinal follow-up and outcomes among a
population with chronic kidney disease in a
large managed care organization. Arch Intern Med
2004164659663.
42
Correlation between decline in kidney function
(estimated by GFR) and increasing incidence of CV
complications death from CV disease
GFR (mL/min/1.73 m2)Blue gt 75.0 Yellow
60.074.9 Green 45.059.9 Purple lt 45
43
Ca2 Phosphorus Homeostasis
- Abnormalities in Ca2 phosphorus metabolism
typically occur in CKD stages 3, 4, 5 - 2 hyperparathyroidism can develop at GFR lt 80
mL/min/1.73 m2 despite normal Ca2 phosphorus
levels - Monitor parathyroid hormone concentration (PTH),
vitamin D, Ca2, phosphorus starting in stage 3
CKD - Ca2, phosphorus, PTH correction may reduce CV
risk - Phosphate binders AlOH, calcium carbonate,
calcium acetate, lanthanum carbonate, sevelamer
Martinez I, Saracho R, Montenegro J, Llach F. The
importance of dietary calcium and phosphorous in
the secondary hyperparathyroidism of patients
with early renal failure. Am J Kidney Dis
199729496502.
National Kidney Foundation. K/DOQI clinical
practice guidelines for managing dyslipidemias in
chronic kidney disease. Am J Kidney Dis
200341S1S92.
44
(No Transcript)
45
Anorexia Malnutrition
- Limited data defining CKD stage where
malnutrition develops - NKF K/DOQI guidelines evaluate for signs of
malnutrition when GFR lt 60 mL/min/1.73 m2 - stages 3, 4, 5
Kopple JD. National kidney foundation K/DOQI
clinical practice guidelines for nutrition in
chronic renal failure. Am J Kidney Dis
200137S66S70.
46
Anorexia Malnutrition
- Nutrition assessment
- dietary protein
- calorie intake
- serum albumin
- urine protein
Kopple JD. National kidney foundation K/DOQI
clinical practice guidelines for nutrition in
chronic renal failure. Am J Kidney Dis
200137S66S70.
47
Treatment Goals
- Delay progression
- Minimize complications
- modest dietary protein restriction may be
beneficial - pharmacologic therapy control underlying
conditions - (e.g. DM, HTN) prevent functional decline
- Generally requires multimodality treatment
- ACEIs /or ARBs key therapeutic component for
most patients
48
Nonpharmacologic Therapy
- Dietary Protein Restriction
- experimental animal studies suggest dietary
protein restriction delays rate of decline in
kidney function - Modification of Diet in Renal Disease (MDRD)
- randomized controlled trial randomized by
dietary protein intake BP - evaluated benefit of dietary protein restriction
BP reduction on CKD progression - subjects with moderate CKD (GFR 25 to 55
mL/min/1.73 m2)
Brenner BM. Hemodynamically mediated glomerular
injury and the progressive nature of kidney
disease. Kidney Int 198323647655.
Levey AS, Adler S, Caggiula AW, et al. Effects of
dietary protein restriction on the progression of
advanced renal disease in the Modification of
Diet in Renal Disease Study. Am J Kidney Dis
199627652663.
49
MDRD
- Mean follow-up 2.2 years protein restriction
did not show benefit in slowing CKD progression
in 1 analysis - 2 analysis (patients compliant with dietary Rx)
- GFR lt 25 mL/min/1.73 m2
- protein intake of 0.6 g/kg/day associated with
decreased rate of progressive renal disease - different statistical method from primary
analysis - progression to ESRD reduced by 41 for each 0.2
g/kg/day reduction in dietary protein intake
Levey AS, Adler S, Caggiula AW, et al. Effects of
dietary protein restriction on the progression of
advanced renal disease in the Modification of
Diet in Renal Disease Study. Am J Kidney Dis
199627652663
50
Nonpharmacologic Therapy
- Data suggest small benefit from dietary protein
restriction - Low protein diets may lead to malnutrition with
advanced CKD nephrotic-range proteinuria - NKF K/DOQI advocates dietary protein 0.6
g/kg/day for patients with GFR lt 25 mL/min/1.73
m2 - Titrate protein intake to 0.75 g/kg/day when
patients cannot achieve or maintain adequate
nutritional status with lower-protein diet (0.6
g/kg/day)
Kopple JD. National kidney foundation K/DOQI
clinical practice guidelines for nutrition in
chronic renal failure. Am J Kidney Dis
200137S66S70.
51
Treatment Diabetic CKD
- CKD treatment guidelines recognize differences in
pathogenesis course of diabetic/nondiabetic CKD - BP reduction in type 1 type 2 DM patients
reduces rate of CKD progression - Benefit of BP control confirmed in studies of
type 2 DM patients with microalbuminuria - using an ACEI or ARB
- likely beneficial nonhemodynamic effects on CKD
progression - BP lowering effects as well
52
Effects of Antihypertensives on Renal Blood Flow
(RBF) Glomerular Filtration Rate (GFR)
Antihypertensive Agent Mechanism of Action Effects on Renal Hemodynamics
ACE inhibitors/ARBs Reduce intraglomerular pressure Decrease sodium and volume retention Preserve GFR Decrease GFR, RBF
Diuretics Sodium and volume depletion Increase vasodilatory prostaglandin levels (IV loop diuretics) Renal vasoconstriction (IV thiazide diuretics) Decrease GFR, RBF Increase RBF Decrease GFR, RBF
ß-Adrenergic blockers Decrease Cardiac output Increase renal vascular resistance (nonselective agents) Increase renal vascular resistance (ß1-selective agents) Decrease GFR, RBF Decrease GFR, RBF No change in GFR, RBF
Centrally acting antiadrenergic drugs Decrease renal vascular resistance (methyldopa) Decrease renal perfusion pressure (clonidine, a2-adrenergic agonist) No change in GFR, RBF Decrease GFR, RBF
Peripherally acting antiadrenergic drugs Direct vasodilation (postsynaptic a1-adrenoreceptor blocking agents) No change in GFR, RBF
Direct vasodilator agents Decrease renal vascular resistance (hydralazine, minoxidil) Arterial vasodilation plus dilatation of venous capacitance vessels (nitroprusside) Increase RBF, no effect on GFR Decrease GFR RBF (acute effect)
Calcium channel blockers Decrease renal vascular resistance by vasodilation of afferent arterioles (hypertensive patients) Increase RBF, no change in GFR
DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells
BG, Posey LM Pharmacotherapy A Pathophysiologic
Approach, 7th Edition http//www.accesspharmacy.c
om
53
HTN Control in DM CKD
- JNC 7 goal BP lt 130/80 mm Hg for CKD patients
- gt 3 antihypertensives generally required BP
often difficult to control - HTN DM 6 fold higher ESRD risk than patients
with DM alone - BP control reduces GFR decline albuminuria in
hypertensive DM patients - ACEIs reduce glomerular capillary pressure
volume preserve renal function
Chobanian AV, Bakris GL, Black HR, et al. Seventh
report of the Joint National Committee on
Prevention, Detection, Evaluation, and Treatment
of High Blood Pressure. Hypertension
20034212061252.
Bakris GL, Williams M, Dworkin L, et al.
Preserving renal function in adults with
hypertension and diabetes A consensus approach.
National Kidney Foundation Hypertension and
Diabetes Executive Committees Working Group. Am J
Kidney Dis 200036646661.
54
CONTINUED ON NEXT SLIDE
55
CONTINUED FROM PREVIOUS SLIDE
56
Antihypertensives - ACEIs
- Beneficial effects on renal function (patients
DM) - both type 1 2 DM
- different degrees of kidney damage
- ACEI therapy
- begin at a low dose increase dose at 4-week
intervals to reduce microalbuminuria (even
normotensive patients) - antiproteinuric effects not necessarily attained
at antihypertensive doses - increase dose until proteinuria reduced by 30 to
50 - titration limited by adverse effects elevated
SCr K
57
ELITE Trial
- The Evaluation of Losartan In The Elderly (ELITE)
- Losartan vs captopril in diabetics nondiabetics
- Comparable renal benefits of both ARBs ACEIs in
HF patients - Shows efficacy of both ACEIs ARBs in type 2 DM
- Only ACEIs adequately evaluated in type 1 DM
patients
Pitt B, Segal R, Martinez FA, et al. Randomised
trial of losartan versus captopril in patients
over 65 with heart failure (Evaluation of
Losartan in the Elderly Study, ELITE). Lancet
1997349747752.
Hostetter TH. Prevention of end-stage renal
disease due to type 2 diabetes. N Engl J Med
2001345910912.
58
CALM Study
- Candesartan And Lisinopril Microalbuminuria
(CALM) - Evaluated ACEI/ARB monotherapy combination
therapy in type 2 DM patients - 12 to 24 week study
- 3 groups
- lisinopril 20 mg/day
- candesartan 16 mg/day
- combination of both
Mogensen CE, Neldam S, Tikkanen I, et al.
Randomised controlled trial of dual blockade of
renin-angiotensin system in patients with
hypertension, microalbuminuria, and non-insulin
dependent diabetes The Candesartan and
Lisinopril Microalbuminuria (CALM) study. BMJ
200032114401444.
59
CALM Study
- Greater reduction in urinary albumin-to-creatinine
ratio with combination therapy (50) - lisinopril alone (39)
- candesartan alone (24)
- Significantly greater BP reduction with
combination - Unclear if combination enhances antiproteinuric
effect or if albumin-to-creatinine ratio
reduction attributable to greater BP reduction
Mogensen CE, Neldam S, Tikkanen I, et al.
Randomised controlled trial of dual blockade of
renin-angiotensin system in patients with
hypertension, microalbuminuria, and non-insulin
dependent diabetes The Candesartan and
Lisinopril Microalbuminuria (CALM) study. BMJ
200032114401444.
60
CKD Patients With HTN
- No ACEI shown to be superior to any other ACEI
- 1 goal treat BP to target
- 2 goal control proteinuria
- Antihypertensive ceiling effect for ACEI dose
titration not confirmed for lowering urinary
protein excretion - ACEIs generally more cost-effective than ARBs
- Adverse effects with an ACEI switch to an ARB
may be appropriate
Kshirsagar AV, Joy MS, Hogan SL, Falk RJ,
Colindres RE. Effect of ACE inhibitors in
diabetic and nondiabetic chronic renal disease
A systematic overview of randomized
placebo-controlled trials. Am J Kidney Dis
200035695707.
61
Nondihydropyridine CCBs
- Diltiazem/verapamil decrease glomerular injury
without negatively changing renal hemodynamics - May have beneficial effects on proteinuria
similar to ACEIs - Studies suggest efficacy of combination therapy
with ACEIs nondihydropyridine CCBs may be
superior in proteinuria reduction than either
agent alone - Generally 2nd line when ACEIs or ARBs not
tolerated
Dworkin LD, Benstein JA, Parker M, Tolbert E,
Feiner HD. Calcium antagonists and converting
enzyme inhibitors reduce renal injury by
different mechanisms. Kidney Int 199343808814.
Epstein M. Effects of ACE inhibitors and calcium
antagonists on progression of chronic renal
disease. Blood Press Suppl 19952108112.
62
Clinical Controversy
- ONgoing Telmisartan Alone and in combination with
Ramipril Global Endpoint Trial (ONTARGET) - 1 endpoint composite of death, dialysis, SCr
doubling - Prospective, randomized, multicenter,
double-blind trial - randomized patients to ramipril, telmisartan, or
combination of both - 25,620 patients age gt 55 yr with diabetes
end-organ damage or established atherosclerotic
vascular disease - Combination therapy reduces proteinuria more than
monotherapy but worsens major renal outcomes
Mann JF, Schmieder RE, McQueen M, et al. Renal
outcomes with telmisartan, ramipril, or both, in
people at high vascular risk (the ONTARGET
study) a multicentre, randomised, double-blind,
controlled trial. Lancet 2008372547-543.
63
Non-diabetic Patients
- BP reduction key to decreasing CV renal
complications - Antihypertensive agents not equal in kidney
function preservation despite similar BP
reduction - ACEIs ARBs 1st line in CKD patients because
they reduce intraglomerular pressure
64
Antihypertensives ACEIs
- BP reductions done over weeks to allow the kidney
to adapt to reduced perfusion pressures - Typically acute but sustained 25 to 30 GFR
reduction - 3 to 7 days after ACEI initiation
- reduced intraglomerular pressure
- If sustained SCr increase gt 30, consider
discontinuation - Monitor for hyperkalemia, acute GFR reduction
Chobanian AV, Bakris GL, Black HR, et al. Seventh
report of the Joint National Committee on
Prevention, Detection, Evaluation, and Treatment
of High Blood Pressure. Hypertension
20034212061252.
Apperloo AJ, de Zeeuw D, de Jong PE. A short-term
antihypertensive treatment-induced fall in
glomerular filtration rate predicts long-term
stability of renal function. Kidney Int
199751793797.
65
Antihypertensives ARBs
- ARBs have similar efficacy to ACEIs for kidney
protection in patients with several forms of
glomerulonephritis - Proteinuria reduction 25 to 47
- Most clinicians use ACEI/ARB therapy in patients
with nondiabetic CKD proteinuria
66
Antihypertensives ARBs
- Selection of ACEIs vs ARBs
- cost of therapy
- patient tolerance
- clinician preference
67
Antihypertensives CCBs
- Effective for HTN in patients with nondiabetic
CKD - Only nondihydropyridine CCBs shown to reduce rate
of renal function decline - No data to suggest higher doses needed to reduce
proteinuria compared to antihypertensive doses
68
Antihypertensives Others
- Diuretics commonly used to treat fluid overload
HTN no compelling data to suggest renal
protection - Can use central peripherally acting
antihypertensive agents in CKD patients - Consider dose reductions for renal impairment
/or supplemental doses due to dialysis removal
of hydrophilic ß-blockers - nadolol
- acebutolol
- atenolol
69
Smoking Cessation
- Adverse effects of smoking
- acute GFR reduction
- nicotine
- ? urinary albumin excretion
- ? BP
- ? HR
- Educate patients regarding risks
- Institute appropriate therapeutic options
70
Anemia Management
- Anemia may increase rate of CKD progression
- Cardiorenal anemia syndrome" describes
interrelationship between anemia, HF, CKD - Erythropoietin stimulating agents
- higher target Hgb (13.o to 15.0 mg/dL) increases
CV risk without improving quality of life - target Hgb 10.5 to 11.5 mg/dL associated with
fewer CV events than target Hgb level in the
normal range
Drueke TB, Locattelli F, Clyne N, et al.
Normalization of hemoglobin level in patients
with chronic kidney disease and anemia. N Engl
J Med 20063552071-84.
Siiningh AAK, Szczech L, Tang KT, et al.
Correction of anemia with epoetin alpha in
chronic kidney disease and anemia. N Engl J Med
20063552085-98.
71
Costs of CKD Treatment
- High financial societal costs
- 0.5 of total Medicare population accounts for 5
of Medicare expenditures - Annualized expenditures per beneficiary
- 36,000 for patients lt 24 years of age
- 51,000 for patients gt 75 years of age
- Costs for care of advanced CKD estimated to
increase dramatically over the next decade - 28 billion dollars by 2010 for Medicare alone
USRDS. USRDS 2001 Annual Data Report. Bethesda,
MD National Institutes of Health, National
Institute of Diabetes and Digestive and Kidney
Disease, 2001.
72
Conclusions DM Patients
- Pharmacologic interventions limit CKD progression
- Screening for microalbuminuria
- type 1 DM patients 5 years after diagnosis
- type 2 DM patients annually
- urinary albumin excretion or urinary
albumin-to-creatinine ratio - Maintain blood glucose close to the normal range
Standards of medical care in diabetes2007.
Diabetes Care 2007200130(Suppl 1)S4S41.
73
Conclusions DM Patients
- 1st Line ACEI therapy
- persistent microalbuminuria 30 to 300 mg/day
- overt albuminuria gt 300 mg/day
- even if not hypertensive
- titrate to maximal reduction in urinary albumin
excretion - evaluate SCr K within 1 wk of initiation/dose
change
74
Conclusions DM Patients
- ARBs
- another 1st line therapy in type 2 DM patients to
reduce persistent proteinuria, albuminuria - Nondihydropyridine CCBs
- may be effective 2 agent in patients unable to
tolerate ACEI or ARB
75
Conclusions DM Patients
- Combination ACEI/ARB may result in greater
proteinuria or albuminuria reduction than either
agent alone - may be alternative for patients that are not
maximally responding to single-agent therapy - Aldosterone receptor blocker consider for
subjects with documented aldosterone escape
76
Diabetic Patients
DM Patients
77
Diabetic Patients
DM Patients
78
Conclusions Non-DM Patients
- Monitor nutrition frequently
- MDRD study
- moderate renal dysfunction GFR 25 to 55
mL/min/1.73 m2 - low-protein diet of variable benefit
- standard-protein diet reasonable unless rapid
disease progression - severe renal dysfunction GFR 13 to 24
mL/min/1.73 m2 - low-protein diet (0.6 g/kg/day) may reduce rate
of renal function decline, time to reach
end-stage kidney disease, onset of uremic
symptoms
Jacobson HR, Striker GE. Report on a workshop to
develop management recommendations for the
prevention of progression in chronic renal
disease. Am J Kidney Dis 199525103106.
Levey AS, Adler S, Caggiula AW, et al. Effects of
dietary protein restriction on the progression of
advanced renal disease in the Modification of
Diet in Renal Disease Study. Am J Kidney Dis
199627652663.
79
Non-diabetic Patients
80
Non-diabetic Patients
81
Conclusions Non-DM Patients
- BP goal lt 130/80 mm Hg
- CKD proteinuria gt 3 g/day
- 1st line ACEI or ARB
- treat hyperlipidemia to reduce CV risk
82
Conclusions Non-DM Patients
- CKD stage 4 prepare patients for
renal-replacement therapy - discuss hemodialysis, peritoneal dialysis, renal
transplant - early referral to clinician specializing in care
of CKD patients (e.g. nephrologist) - dialysis vascular access placement
- evaluate for uremia symptoms
- Identify/treat metabolic abnormalities
Eknoyan G, Levin N. NKF-K/DOQI Clinical Practice
Guidelines Update 2000. Foreword. Am J Kidney
Dis 200137S5S6.
83
Acknowledgements
- Prepared By/Series Editor April Casselman,
Pharm.D. - Editor-in-Chief Robert L. Talbert, Pharm.D.,
FCCP, BCPS, FAHA - Chapter Authors Melanie S. Joy, Pharm.D., FCCP
- Abhijit Kshirsagar, MD, MPH
- Nora Franceschini , MD, MPH
- Section Editor Gary R. Matzke, Pharm.D.
Recommended
CrystalGraphics Presentations





























