
Background - PowerPoint PPT Presentation
1 / 1
Title:
Background
Description:
... a primary or secondary cause of death from the Ohio and Kentucky departments of ... death certificate databases and the national Social Security Death Index. ... – PowerPoint PPT presentation
Number of Views:32
Avg rating:3.0/5.0
Title: Background
1
Long-Term Mortality After Ischemic Stroke
Effect of Diabetes in the Greater
Cincinnati/Northern Kentucky Stroke Study
Brett Kissela, Jane Khoury, Kathleen Alwell,
Rosie Miller, Irene Ewing, Dawn Kleindorfer, Alex
Schneider, Daniel Woo, James Gebel, Jerzy
Szaflarski, Charles Moomaw, Rakesh Shukla, Joseph
Broderick The Neuroscience Institute University
of Cincinnati Department of Neurology
Louisville, KY
- Background
- We have previously utilized the Greater
Cincinnati/Northern Kentucky Stroke Study, a
population-based epidemiologic study, to examine
characteristics of stroke in patients with
diabetes. We have demonstrated significant
differences in ischemic stroke incidence rates by
age, with significantly higher ischemic stroke
risk in younger age groups. We have also shown
significant differences in patient
characteristics, where diabetic stroke patients
are younger, more likely to be African-American,
and more likely to have risk factors of
hypertension, cardiac disease, and high
cholesterol. In our population, diabetic patients
with ischemic stroke have worse functional
outcomes but similar case-fatality rates at 30
days, 90 days, and 1 year as compared to
non-diabetic patients. - This analysis was undertaken to determine
how diabetes affects long-term mortality after
ischemic stroke. One previous study from Sweden
reported 71 mortality by 9 years in 121 ischemic
stroke patients with diabetes (Olsson, et.al.,
Diabetologia, 33244-2491990). Larger studies of
long-term mortality after ischemic stroke which
examine the effect of diabetes have not been
performed. - Methods
- Study population all residents of the Greater
Cincinnati/Northern Kentucky region, including
two southern Ohio counties and three contiguous
Northern Kentucky counties that abut the Ohio
River. Although residents of nearby counties seek
care at the 19 acute care hospitals in the study
region, only residents of the 5 study area
counties are included as cases (identified as
being from the study area based on their zip
code) (Figure 1). - Phase 1 collection of African American strokes
between 1/1/93-6/30/93 - Phase 2 collection of all strokes in the study
population between 7/1/93-6/30/94.
- Limitations
- Very crude measures of stroke severity were used.
- No data were collected about medical
complications after stroke and no measure of
medical comorbitidies was used. - Undiagnosed diabetes may bias survival in the
non-diabetic patients. This is true for each
risk factors considered. In some cases this bias
is caused by poor documentation in the medical
record, such that we not able to record a
diagnosis that had been established. In other
cases, the patient may have had a diagnosis made
only after stroke, which we would not capture. - Conclusions
- Increasing age and stroke severity, higher
pre-stroke mRS, diabetes, male gender, and
smoking are associated with increased post-IS
mortality. - A history of high cholesterol and moderate
alcohol use are associated with decreased
mortality. - Ischemic stroke patients with diabetes in our
population had higher mortality at every time
point after stroke and 85 mortality by 9 years,
although a statistical difference was not seen
until after the first year. - The reasons for increased mortality and worse
functional outcomes after ischemic stroke in
diabetic patients require further study.
Outpatient (in Phase 2 only) ascertained via
monitoring of all visits to emergency
departments, public health clinics,
hospital-based outpatient clinics, and family
practice centers, as well as monitoring for
outpatient strokes in a random sample of 50 of
878 primary care physicians offices and 25 of
193 nursing homes. Data Collected the study
nurse performed a comprehensive medical record
abstraction regarding stroke hospitalization and
obtained all available neuroimaging studies.
Classification of race was as self-reported in
the medical administrative record. Classification
of risk factors was based upon a previous
diagnosis as documented in the patients medical
record. Laboratory values were recorded in the
medical record abstract. All borderline cases
were abstracted for physician review to ensure
complete case ascertainment. Case
Inclusion/Exclusion Ultimately, a study
physician reviews each abstract and decides if a
stroke or TIA occurred. Study physicians also
review available neuroimaging and characterize
imaging findings. The physician assigns stroke
subtype and mechanism to each patient based on
all available information, using definitions
previously reported. Cases of ischemic
stroke or TIA in African-Americans between
1/1/93- 6/30/94 and Caucasians between
7/1/93-6/30/94 were used for this
analysis. Statistical analyses Vital status
information for ischemic stroke patients from
7/93-6/94 (n 1909, 30 with diabetes) was
obtained from Ohio and Kentucky death certificate
databases and the national Social Security Death
Index. Mortality was analyzed using a Cox
proportional hazards model.
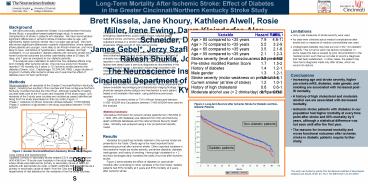
Figure 2. Long-term Survival after Ischemic
Stroke for Diabetic and Non-Diabetic Patients
Non-diabetic patients
Results Variables for predicting mortality
retained in the survival model are presented in
the Table. Clearly age is the most important
factor determining survival after ischemic
stroke. Other important variables in the
predictive model are stroke severity, pre-stroke
disability, diabetes, male gender, and history of
smoking. Having high cholesterol or beverages daily increased the odds of survival
after ischemic stroke. Figure 2
demonstrates the effect of diabetes on
post-stroke mortality after controlling for other
variables in the final model diabetic patients
had 55 mortality at 5 years and 85 mortality at
9 years after ischemic stroke.
- Hospitals
Diabetic patients
Figure 1. Greater Cincinnati/Northern Kentucky
Stroke Study Region
This study was funded by grants from the National
Institutes of Neurological Diseases and Stroke
(Grant s RO-1 NS 30678 and K-23 NS 45054
Recommended
CrystalGraphics Presentations





























