
Background - PowerPoint PPT Presentation
1 / 53
Title: Background
1
(No Transcript)
2
(No Transcript)
3
(No Transcript)
4
Background
- Autism is a Pervasive Developmental Disorder that
results from damage to the central nervous
system. - Characterized by three main behavioral
dysfunctions - 1)impaired social interactions
- 2) difficulty communicating (verbal and
non-verbal) - 3) repetitive interests.
5
Autistic Brain
6
An Autistic Brain result or causeof autism?
- Larger frontal lobes due to excess white matter
Corpus Collosum is undersized Amygdala is
enlarged - 10 larger hippocampus. This region is
responsible for memory. ASD patients rely on
memory to interpret situations - Cerebellum is larger also due to excess white
matter - Too many cables within local areas but not enough
linking different regions
7
Genetic Causes
- Caused by disruptions of the NLGN4 gene on
chromosome Xp22 thus interrupting essential
synaptic function - Maternally inherited duplications of 15q11-q13
- Dozens of genes thought to be implicated
8
Other Possible Causes
- vaccine reactions
- atypical growth in the placenta
- abnormal tissue in the gut
- inflamed tissue in the brain
- food allergies
- disturbed brain wave synchrony
- Some clinicians are using genetic test results to
- recommend unconventional nutritional therapies,
and others employ drugs to fight viruses and
quell inflammation.
9
Autism is an environmentallytriggered problem.
- If it is environmental, then it is treatable and
preventable. - It is NOT HOPELESS and lifelong.
- It is HOPEFUL, with a possible cure.
10
Autism isa whole-body problem.
- Immunological dysregulation with a unique
inflammatory bowel disease - Oxidative stress, systemic inflammation, and
severely disordered urine and serum chemistries
including elevated porphyrins - Decreased methylation capacity, limited
transsulfuration and glutathione deficiency - Increased toxic body burdens primarily of heavy
metals esp. mercury and lead - Chronic viral, fungal and bacterial infections
- Central nervous system hypofusion/abnormal
regulation of blood supply to the brain
Microglial activation, lipid peroxidation,
mitochondrial dysfunction, inactive enzyme
systems.
11
(No Transcript)
12
What is Autism?
- Autism is one of a group of disorders known as
autism spectrum disorder (ASD) - ASDs are developmental disabilities that cause
substantial impairment in three areas of
dysfunction - 1 Qualitative impairment in reciprocal
communication - 2 Impairment of reciprocal social interaction
- 3 Restrictive range of play and interests
- 4 Neurodevelopmental disorder with a spectrum of
clinical conditions
13
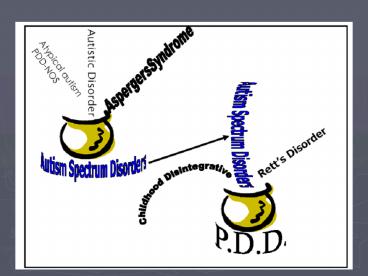
DSM-IV ClassificationPervasive Developmental
Disorders
14
ASD Facts
- Present at birth
- Onset of symptoms before 36 months
- Accurate diagnosis possible at 18-24 months
- Parents first voice concerns 18 months
- Diagnosis is typically 3 years or older
15
(No Transcript)
16
(No Transcript)
17
(No Transcript)
18
ASD Facts Epidemiology
- Prevalence between 1166 - 500
- ASD more prevalent in pediatric population than
Cancer, Diabetes Downs Syndrome - Male to female ratio 4 to 1
19
(No Transcript)
20
ASD Facts Causes
- Causation unknown
- Strong genetic influence
- Identical twin studies show 75 risk
- Recurrence risk in siblings 2-8
21
(No Transcript)
22
What are the earliestsigns of Autism?
- Delays or abnormalities in
- 1 Joint Attention
- 2 Social Interaction
- 3 Play Behavior
23
Typical DevelopmentJoint Attention
24
Typical DevelopmentSocial Interaction
25
Typical DevelopmentPlay Behavior
26
Why screen for autistic spectrum disorders in
primary care?
- Prevalence is high
- Condition is serious
- Effective intervention. There is improved
outcomes with early and intense interventions - Tools now available
- Parents expect and want it
27
Screening Tools
- What screening tools can do
- identify children who might have developmental
delays. - Be specific to a disorder or an area be general
- What screening tools cannot do
- Give sure evidence of developmental delays
- Be used to make a diagnosis
28
Developmental and SocialEmotional Screening
- Consider using a standardized parent report tool
at every well child visit - Examples include
- Parental Evaluation of Developmental Status
- (PEDS)
- Ages Stages Questionnaire (ASQ)
- Ages Stages Questionnaire Social Emotional
- (ASQSE)
- Modified CHecklist for Autism in Toddlers
- (M-CHAT
29
Listen to Parents
- Parents
- Are aware of the possibility of autism
- Do have concerns when something is wrong
- Do give accurate and reliable information about
their children - Need your questions to generate discussion about
their childs development
30
Early RED Flags forAutism
- No big smiles or other warm, joyful expressions
by - 4-5 months
- No back-and-forth sharing of sounds by 9 months
- No babbling at 12 months
- No back-and-forth gestures, such as pointing,
reaching, or waving by 12 months - No words by 16 months
- No two word spontaneous meaningful phrases by 24
months
31
Autism- presentingsymptoms
- Speech delay
- Expressive skills may appear more advanced than
receptive - Poor eye contact
- Lack of joint attention-gaze
- Lack of use of gestures
- Lack of pretend play
- Behavioral problems-often appear hyperactive
- Repetitive behaviors emerge around three years
old - Hand finger mannerisms
- Abnormal processing and modulation of sensory
stimuli
32
Language Delay
- Absolute indications for immediate evaluation
- 9 months No babbling
- 12 months No pointing or other gestures
- 16 months No single words
- 24 months No functional 2-word phrases (not
echolalic) - Any age Any loss of language or social skills
33
Autism Assessment18 36 months
- Deficits are more important than the presence of
specific behaviors
34
Autism Assessment18 36 months
- Lack of
- Use of eye contact to regulate social interaction
- Orienting to name
- Joint attention behaviors pointing showing
- Pretend play
- Imitation
- Nonverbal communication
- Language development
35
Autism Assessment18 36 months
- Autism screening tools are not recommended for
primary care setting - At 18-month visit use parent questioning and
direct observation to assess child for - Refer for further evaluation if concerned
36
Sorting out the truth fromautism stereotypes
37
Autism AssessmentStaff Roles
- Front office staff
- Maintain and update referral list
- Provide information on logistics of referral
- Allied health professionals
- Distribute patient education
- Provide routine feedback
- Clinical providers
- Observe childs behavior
- Listen to parents concerns
- Advise parents on development and behavior
- Make referrals
38
Autism AssessmentReimbursement
- Autism assessment with observation and parental
discussion falls under the general well child
visit code - Implement standardized developmental screening to
increase reimbursement
39
Referrals for children whoshow signs of autism
- DO NOT DELAY
- Under 3 years refer to Early Intervention
- 3 years or above refer to School District
- For diagnostic confirmation consider
- Medical Diagnostic
- Developmental behavioral pediatrician
- Child psychologist
- Pediatric neurologist
- Child psychiatrist
40
0 3 Early Intervention
- Functions
- Assist in screening/evaluation
- Determine eligibility
- Assess needs
- Plan for services
- Identify providers
41
Autism Intervention
- Issues to consider when choosing a treatment
plan - Evidence-based
- Cost
- Time
- Family involvement
42
3 21Special Education
- Mandated by federal IDEA legislation
- Programs managed and vary by school district
- Make referrals in writing!
- Individualized Education Plan (IEP) for each
child - Services for children with autism may include
- Speech therapy
- Occupational therapy
- Communication assistance (PECS)
- Teacher education on classroom management
43
Encouraging Next Steps
- Acknowledge parents fear and grief
- Provide information on how to tell others
- Provide parent with information on the referral
sources - Encourage communication
- Set a follow-up appointment
44
Advantage of Early Diagnosis Autism is
treatable Early diagnosis
- leads to early intervention, results in improved
outcome for many children with autism. - Facilitates educational planning
- Provides family support and education
- Early management of family stress and anguish
- Delivery of appropriate medical care and
treatment
45
Epilepsy and Autism
- 20-40 of autistic children have an abnormal EEG
- 30 of all children ultimately develop epilepsy
- Preschool years
- Puberty
- Predictors for epilepsy development
- Degree of mental handicap (severe)
- Severity of autism
- Overt motor deficits (67)
- Etiology of autism
- Regression after age 3
46
Clinical Presentation
- Seizure types complex partial seizures are most
common, /- secondary generalization - Suspect if child has intermittent events of
diminished or lost consciousness lasting seconds
to a few minutes, is not interruptable during
these events or is postictally sleepy or very
confused
47
Non-epileptic events
- History is key to differentiate seizures from
- autistic behaviors
- Staring spells can be interrupted by vigorous
tactile stimulation - Ritualistic behavior usually complex movement,
can interrupt but child often upset, more likely
if child is anxious, overwhelmed - Tantrums provoked by specific situations,
demands on child, often prolonged (child may be
tired afterwards), complex behaviors, child
responds during tantrum
48
Role of EEG
- Often a challenge in autistic children!
- EEGs are frequently abnormal in children without
seizures only do if the clinical suspicion is
high, based on careful history - Sleep-deprived recording more likely to
demonstrate abnormality than routine awake, but
can be difficult to obtain, unless sedation given - Sleep recording essential if CSWS suspected
49
Treatment
- If clinical history very suspicious, even if EEG
unremarkable, treatment should be considered. - Base treatment on seizure type and potential
adverse effects - Use carbamazepine/oxcarbazepine cautiously if EEG
showing frequent centrotemporal spikes may
exacerbate condition - Caution with clobazam, levetiracetam may worsen
behavior
50
With biomedical treatments,there is hope for
recovery.
- Leave no stone unturned
- Address the evidence implicating vaccine
overload, mercury and aluminum from vaccines - When treated biomedically, autistic children get
better - Research and produce successful antioxidant,
methylation and blood brain barrier chelation
treatments as well as immune system,
detoxification and inflammation interventions
51
(No Transcript)
52
Hundreds of thousands of sickchildren are
silently waiting.
- Pursue research and treatments that will impact
the most lives as quickly as possible. - Follow clues provided by evidence-based
treatments. - Institute a translational research protocol where
clinicians who care for children with autism
advise research into the most promising areas of
intervention. - Act with urgency. Follow the truth where ever it
leads.
53
(No Transcript)
Recommended
CrystalGraphics Presentations





























