
CReactive Protein in Sickle Cell Crisis - PowerPoint PPT Presentation
1 / 1
Title:
CReactive Protein in Sickle Cell Crisis
Description:
A central characteristic of sickle cell disease is periods of extreme pain, ... Because of the abnormal shape, sickle cells create a clog in blood vessels. ... – PowerPoint PPT presentation
Number of Views:235
Avg rating:3.0/5.0
Title: CReactive Protein in Sickle Cell Crisis
1
C-Reactive Protein in Sickle Cell Crisis
Georgetown
UNIVERSITY
Mike Blainefield Mary Kate DeLong Laura DiLeo
Roland Dimaya Allan Angerio, Ph. D., School of
Nursing and Health Studies, Georgetown University
INTRODUCTION
HYPOXIA CRESCENT-SHAPED RED BLOOD
CELLS OCCLUSSION OF BLOOD VESSELS ACUTE PHASE
PROTEINS COMPLEMENT C-REACTIVE
PROTEIN PROTEIN
INFLAMMATION SICKLE CELL CRISIS
C-REACTIVE PROTEIN
Sickle cell disease (SCD) is an inherited genetic
disorder of hemoglobin in which abnormal sickle
hemoglobin (Hb SS) partially or completely
replaces normal hemoglobin (Hb AA). A central
characteristic of sickle cell disease is periods
of extreme pain, referred to as crisis, which
involves inflammation due to severe hypoxia and
vaso-occlusion. In response to inflammation, the
liver releases a variety of acute phase proteins.
One such product, C-reactive protein (CRP),
serves as a dominating diagnostic marker of
inflammation in crises. We reviewed studies that
followed levels of CRP in non-SCD patients, SCD
patients in crises, and SCD patients not in
crises. Results show trace levels of C-reactive
protein in SCD patients not in crisis, and highly
elevated levels of CRP in SCD patients in crisis.
Further research may deem CRP a useful tool in
predicting the onset of sickle cell crisis.
C-reactive protein was first discovered by
Tillett and Francis in the blood serum of febrile
patients. CRP has been found to aid in binding
of complement proteins to damaged cells. Since
its discovery, CRP has also been identified as
one of the acute phase reactants or acute phase
proteins (any protein whose concentration in
blood plasma increases by more than 25 in
response to inflammation). Produced in the liver
as one of many responses to acute inflammation,
CRP is generated under the stimulation of
interleukin-1 (IL-1) and interleukin-6 (IL-6),
which exist as stimulatory cytokines. As it is
released into the blood during inflammatory
processes, CRP acts as one of the main diagnostic
markers for inflammation.
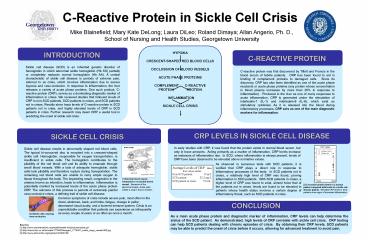
CRP LEVELS IN SICKLE CELL DISEASE
SICKLE CELL CRISIS
In early studies with CRP, it was found that the
protein exists in normal blood serum, but only in
trace amounts. Acting primarily as a marker of
inflammation, CRP levels increase as instances of
inflammation rise. In SCD, where inflammation is
always present, levels of CRP have been observed
to be elevated above normative values.
Sickle cell disease results in abnormally shaped
red blood cells. The typical bi-concaved disc is
morphed into a crescent-shaped sickle cell.
Hemoglobin, responsible for oxygen
transportation, is insufficient in sickle cells.
The hemoglobin contributes to the pliability of
the red blood cell and its ability to emanate
through small blood vessels. With a lack of
adequate hemoglobin, sickle cells lack pliability
and therefore rupture during transportation. The
remaining red blood cells are unable to carry
ample oxygen to tissue throughout the body. The
impending result, congestion in the arteries
known as infarction, leads to inflammation.
Inflammation is potentially marked by increased
levels of the acute phase protein CRP. The
outcome of this process is periods of extremely
painful vaso-occlusive crises, a defining trait
of sickle cell disease.
As observed in numerous tests with SCD patients,
it is verified that CRP plays a direct role in
response to inflammatory processes of the body.
In SCD patients not in crises, a relatively high
level of CRP was found, proving inflammation in
SCD patients. With SCD patients in crises, a
higher level of CRP was found to exist, almost
twice that of the patients not in crises. levels
are found to be elevated in patients whose health
status involves a certain degree of inflammatory
threat, such as SCD patients in crisis.
Average Levels of CRP taken from various
studies Non-SCD patient 10 m/L SCD
patient 32.2 mg/L SCD patient
in crisis 70 m/L
1 Normal blood vessel compared to occluded
blood vessel. Because of the abnormal shape,
sickle cells create a clog in blood vessels..
3 C-reactive protein levels in a normal patient
compared with levels in a sickle cell disease
patient. Elevated CRP levels in SCD patients
show signs of increased inflammation.
Common symptoms of crisis include severe pain,
most often in the chest, abdomen, back, and
limbs, fatigue, change in pallor, decreased
visual acuity, and a lowered immune system.
Crisis is an unpredictable condition that
patients can experience as infrequently as every
couple of years or as often as once a month.
CONCLUSION
2 Sickle cells causing vaso-occlusion.
As a main acute phase protein and diagnostic
marker of inflammation, CRP levels can help
determine the status of the SCD patient. As
demonstrated, high levels of CRP correlate with
sickle cell crisis. CRP testing can help SCD
patients dealing with chronic episodes of crisis.
By obtaining their CRP levels, SCD patients may
be able to predict the onset of crisis before it
occurs, allowing for advanced treatment to avoid
pain.
Sources 1 http//www.clevelandclinic.org/health/
health-info/pictures/sickle.gif 2
http//news.bbc.co.uk/olmedia/1775000/images/_1775
407_sickle_clogs_vessels300.jpg 3
http//www.ebmonline.org/cgi/reprint/230/1/68
Recommended
CrystalGraphics Presentations





























