
Antibiotic Resistant Pathogens in ICU Patients NNIS - PowerPoint PPT Presentation
1 / 40
Title:
Antibiotic Resistant Pathogens in ICU Patients NNIS
Description:
CANADIAN NOSOCOMIAL INFECTION. SURVEILLANCE PROGRAM. 22-34 participating ... Does antibiotic resistance in nosocomial pathogens matter? HEALTH IMPACT OF ... – PowerPoint PPT presentation
Number of Views:585
Avg rating:3.0/5.0
Title: Antibiotic Resistant Pathogens in ICU Patients NNIS
1
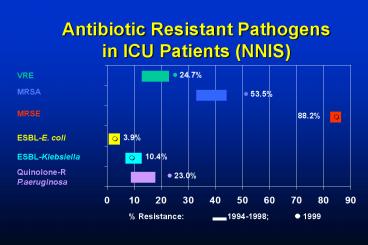
Antibiotic Resistant Pathogensin ICU Patients
(NNIS)
- 24.7
VRE
MRSA
- 53.5
MRSE
88.2
3.9
ESBL-E. coli
?
10.4
ESBL-Klebsiella
?
Quinolone-R P.aeruginosa
- 23.0
Resistance
? 1999
1994-1998
2
(No Transcript)
3
ANTIMICROBIAL RESISTANCE
IN CANADIAN HOSPITALS
4
ANTIMICROBIAL RESISTANCEIN CANADIAN HOSPITALS
- MRSA
- VRE
- ESBLs
5
ANTIMICROBIAL RESISTANCEIN CANADIAN HOSPITALS
- Prevalence
- Epidemiology
- Impact
- Control
6
CHEC/CNISP
- MRSA - prospective since 1995
- VRE - prospective since 1999
- ESBLs - prospective since 2001
7
CANADIAN NOSOCOMIAL INFECTION SURVEILLANCE
PROGRAM
22-34 participating hospitals, 9 provinces 30
teaching hospitals 12 with affiliated
LTCFs 13 with pediatrics 5 pediatric
hospitals LCDC, Health Canada
8
CHEC / CNISP SURVEILLANCEFOR ANTIMICROBIAL
RESISTANCE
- laboratory - based
- prospective, incidence
- updated hospital profiles
- demographic and clinical data
- laboratory characterization, molecular typing
9
MRSA IN CANADA1995-2000
10
MRSA IN CANADA
11
MRSA IN CANADA1995-2000
Eastern Canada
Western Canada
Central Canada
12
MRSA INFECTIONS(1,760 35)
13
MRSA IN CANADAACQUISITION
- 87 acute-care hospital
- 7 long-term care facility
- 6 community
- (excluding 17 unknown)
14
MRSA IN CANADA
- Proportion of hospital-acquired MRSAthought to
have been acquired in theindex hospital 86 - Increase in rate of MRSA acquired inindex
hospital 1997-1999 (plt0.01)1997 - 0.9/1,000
admissions1998 - 1.4/1,000 admissions1999 -
2.8/1,000 admissions
15
MRSA IN CANADAWhy was the culture done?
16
MRSA IN CANADAEpidemiological Link
54 Link
46 No link
17
(No Transcript)
18
Vancomycin-IntermediateS. aureus
- MRSA strains with vancomycinMIC 8µg/ml
- USA, Europe, Japan, Korea,Brazil
- associated with vancomycinuse, and treatment
failure
19
VRE
- approx. 12 of nosocomial enterococcal infections
inU.S. hospitals, 1996 - mostly E. faecium, vanA
- 29 urinary isolates18 wound isolates17
bloodstream isolates
20
VRE IN CANADA(CNISP, 1999)
- 0.9 enterococcal isolates0.54 / 1000
admissions - 83 screening 17 clinical isolates
- 92 patients colonized
21
VRE - ONTARIO
No. patients colonized/infected
718
685
589
445
167
99
2
7
0
22
ESBLs
- 25 K. pneumoniae in hospitalized patients in
France, 1993-1996 - 12 K. pneumoniae in U.S. ICUand 8 non-ICU
patients (Fridkin 1997) - 10 K. pneumoniae 3 E. coliresist to 3rd gen.
cephs U.S. ICUs (NNIS, 1999)
23
ESBLs in Canada
- CNISP survey, 15 labs, 19980.1-0.7 E.
coli0.2-2.5 K. pneumoniae - Saibil et al, 8 Ont. ICUs, 1999-20008/477
(1.7) patients colonized12 Klebsiella 1 E.
coli - Muller et al, outbreak in Ont. LTCFs2000-01
gt140 residents colonizedsmall number of
infections, deaths
24
Does antibiotic resistance in nosocomial
pathogens matter?
25
HEALTH IMPACT OFANTIMICROBIAL RESISTANCE
- Review of 175 reported outbreaks of infection due
to antimicrobial resistant or susceptible
bacteria (S. aureus, Salmonella, Shigella,
Serratia) - Approximately 2X greater mortality,
hospitalization and length of hospital stay
associated with antibiotic resistant infections - - Holmberg, 1987
26
S. AUREUS BACTEREMIA
- Higher mortality associated with MRSA (49-58)
than with MSSA (20-32) - Multivariate logistic regression analysis found
MRSA infection to be an independent risk factor
for mortality(OR, 3.0-4.2) - - Romero-Vivas, 1995
- - Conterno, 1998
27
MORTALITY ASSOCIATED WITHS. AUREUS BACTEREMIA
28
IMPACT OF MRSA/VREDELAYS IN TRANSFER
Mean no. ALC days prior to transfer 130 days
with MRSA/VRE vs. 69 days for matched
controls - Bryce et al, 2000
29
COSTS ASSOCIATEDWITH MRSA
- 14,360/infection for managementof infected
patients - 1,363/admission for managementof colonized
patients
30
VRE BACTEREMIA
- Higher mortality associated withVRE than with
VSE (57 vs. 35 OR 2.1, p0.02) - VRE also associated with moreprolonged
hospitalization(median 17 days vs. 3 days
plt0.001) - - Linden, 1996
- - Vergis, 2001
31
ESBLsImpact
- In most studies, no effect on mortality
- case-control study CAZ-RKlebsiella/E. coli
bacteremia?mortality if appropriate therapynot
started in first 3 days (p0.02)(Schiappa, J Inf
Dis 1996)
32
ESBLs
- 56 of ESBL-producing E. coli and Klebsiella in 2
Philadelphia hospitalswere also resistant to
ciprofloxacinand/or levofloxacin - quinolone resistance in ESBLsassociated with
prior quinoloneuse and residence in a LTCF - Lautenbach, CID 2001
33
STRATEGIES TO MANAGEANTIBIOTIC RESISTANCE
- Surveillance, screening,early detection
- Handwashing and otherinfection control measures
- Appropriate use of antibiotics
- New antimicrobial agents
34
Do control measures work?Can antibiotic
resistance be controlled?
35
MRSA - DENMARK
1966 - 3 1970 - 15 1991 - 2 Control
surveillance screening strict infection
control restricted antibiotic use
36
VRE - ONTARIO
No. patients colonized/infected
718
685
589
445
167
99
2
7
0
37
ESBLsEffect of Control Measures
2. Pena et al, AAC 1998 Setting clonal
outbreak ESBL K. pneumoniae 145 patients
1993-95 Intervention June 1993 - inf. control
measures Sept. 1993 - restricted
oxyimino- ?-lactams Result decreased
no. cases after restricted antibiotic use
38
Pena, AAC 1998
39
ESBLsEffect of Control Measures
3. Lucet et al, CID 1999 Setting French
hospital 140 ESBLs/yr. Intervention ESBL
screening hand hygiene contact
isolation Result ESBL incidence 1992 -
0.56/100 admissions 1995 - 0.06/100 admissions
40
HOW TO ACCOUNT FOR VARIABILITYIN ANTIBIOTIC
RESISTANCE INCANADA VS U.S.A.?
- luck
- different strains
- variability in lab detection
- variability in antibiotic utilization
- variability in infection control practices
Recommended
CrystalGraphics Presentations





























